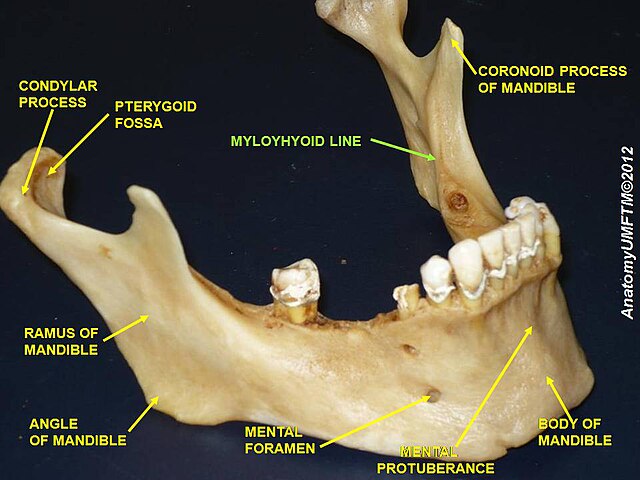
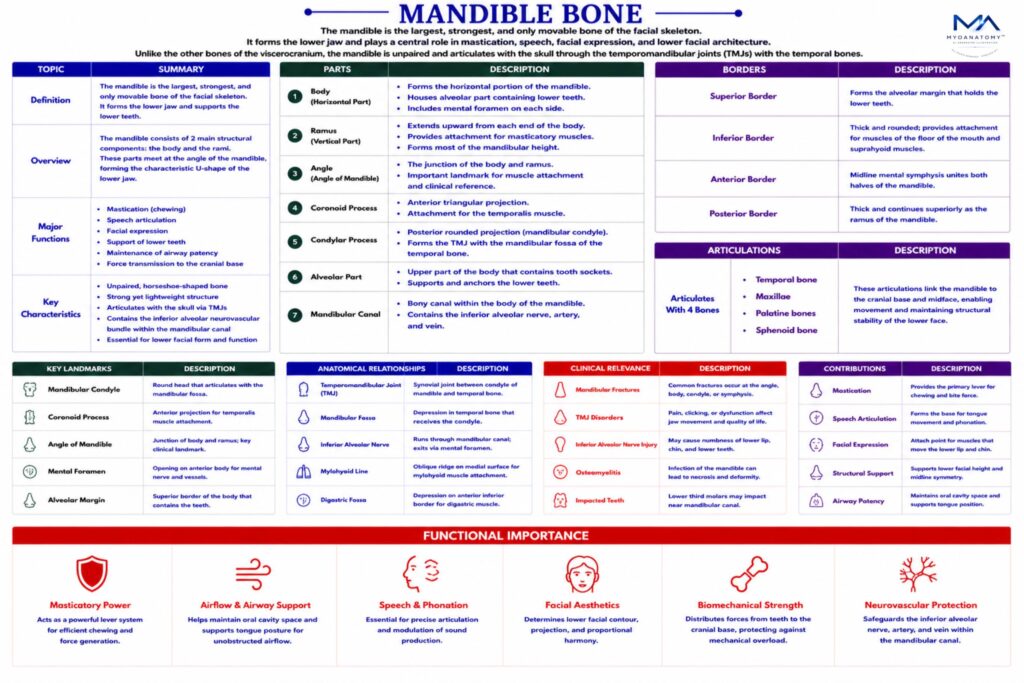
External surface – contains several important anatomical features:
mental protuberance – midline prominence forming the chin
mental tubercles – small elevations on either side of the chin
mental foramen – transmits the mental nerve and vessels, branches of the inferior alveolar neurovascular bundle supplying the lower lip and chin
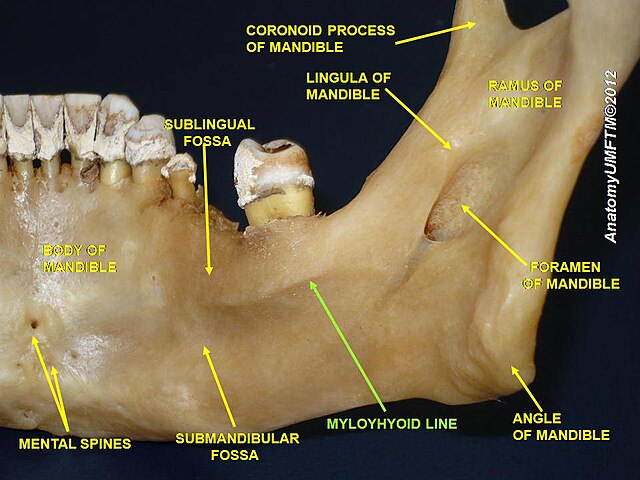
Internal surface– presents important muscular attachments and anatomical landmarks:
mylohyoid line – attachment for the mylohyoid muscle, forming the floor of the oral cavity
digastric fossa – attachment for the anterior belly of the digastric muscle
sublingual fossa – accommodates the sublingual gland
submandibular fossa – accommodates the submandibular gland
Lateral surface- provides attachment for the masseter muscle, one of the primary muscles of mastication.
Medial surface– contains the mandibular foramen, which transmits the inferior alveolar nerve and vessels into the mandibular canal. Just inferior to this foramen is the lingula, a small bony projection serving as attachment for the sphenomandibular ligament. Extending anteriorly from the mandibular foramen is the mylohyoid groove, transmitting the mylohyoid nerve and vessels.