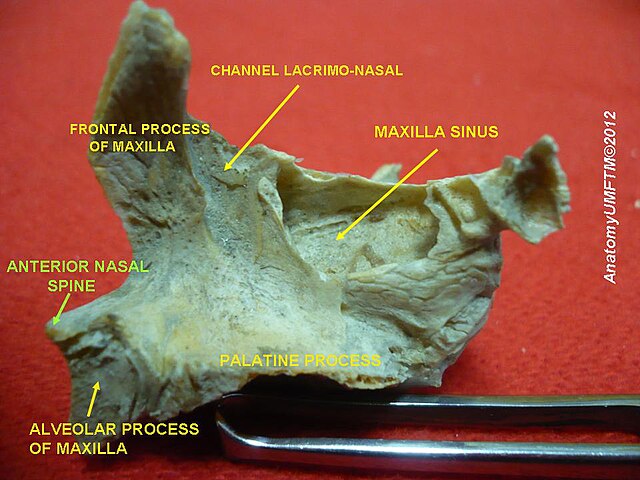
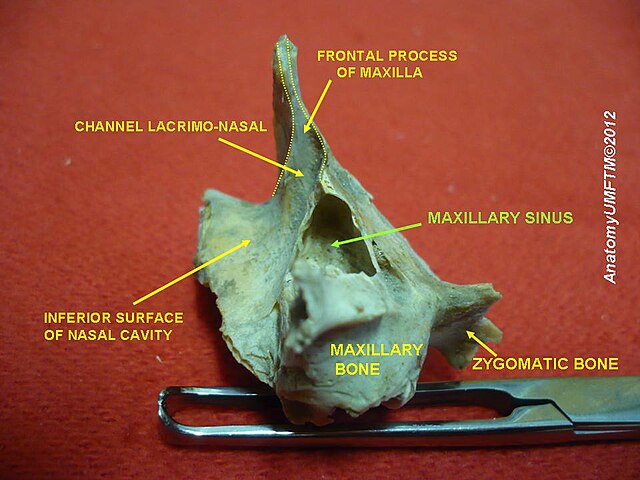
Each maxilla consists of a body and 4 processes:
Frontal Process – extends superiorly to articulate with the frontal bone and contributes to the medial wall of the orbit. It also forms part of the lateral boundary of the nasal cavity.
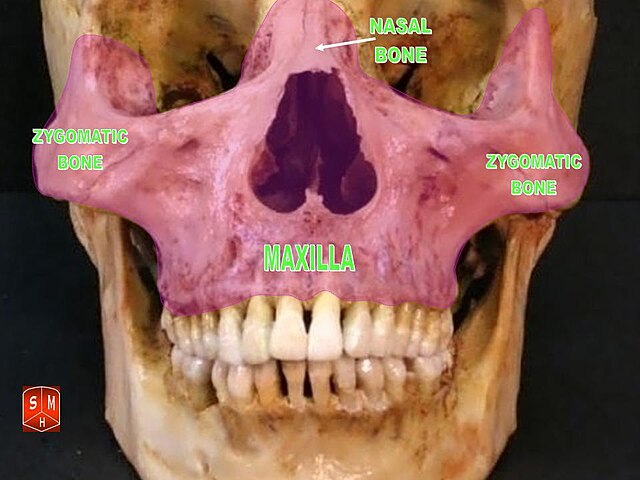
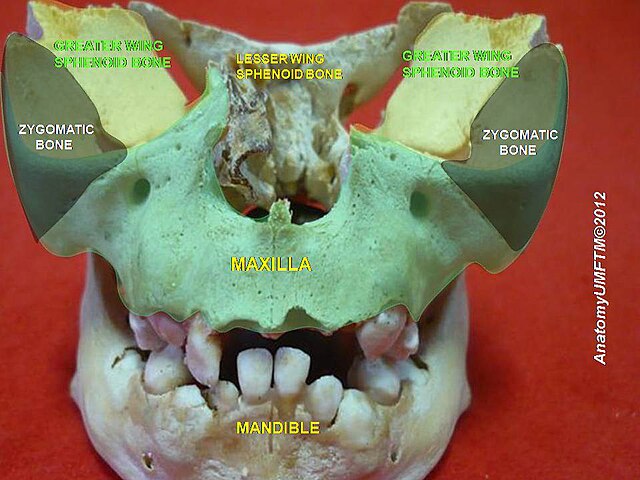
Zygomatic Process – extends laterally and articulates with the zygomatic bone, contributing to the lateral facial skeleton and orbital margin.
Palatine Process – of the two maxillae meet in the midline to form the anterior three-quarters of the hard palate, which separates the oral cavity from the nasal cavity. This structure is essential for speech and swallowing, allowing simultaneous breathing and eating.
Alveolar Process -contains the alveoli, which are sockets that house the roots of the upper teeth. This part of the bone adapts and remodels in response to tooth eruption and loss. These components allow the maxilla to contribute to several anatomical regions of the face.