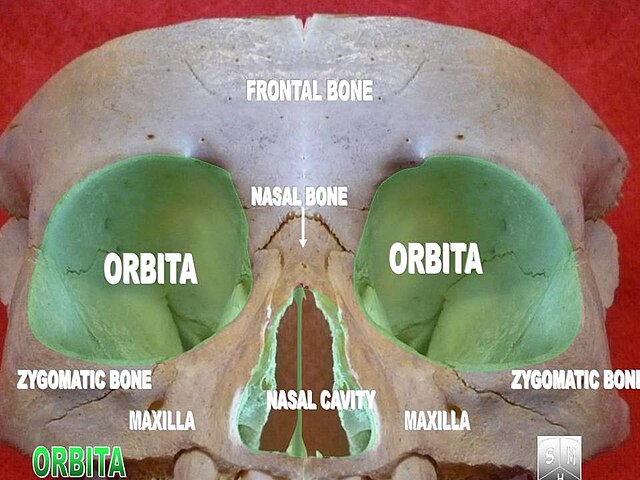
Each orbit provides mechanical protection, structural support, and spatial orientation for the globe while accommodating the extra-ocular muscles, optic nerve, ophthalmic vessels, lacrimal apparatus, and connective tissues that enable precise visual function.
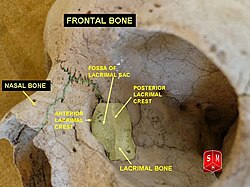
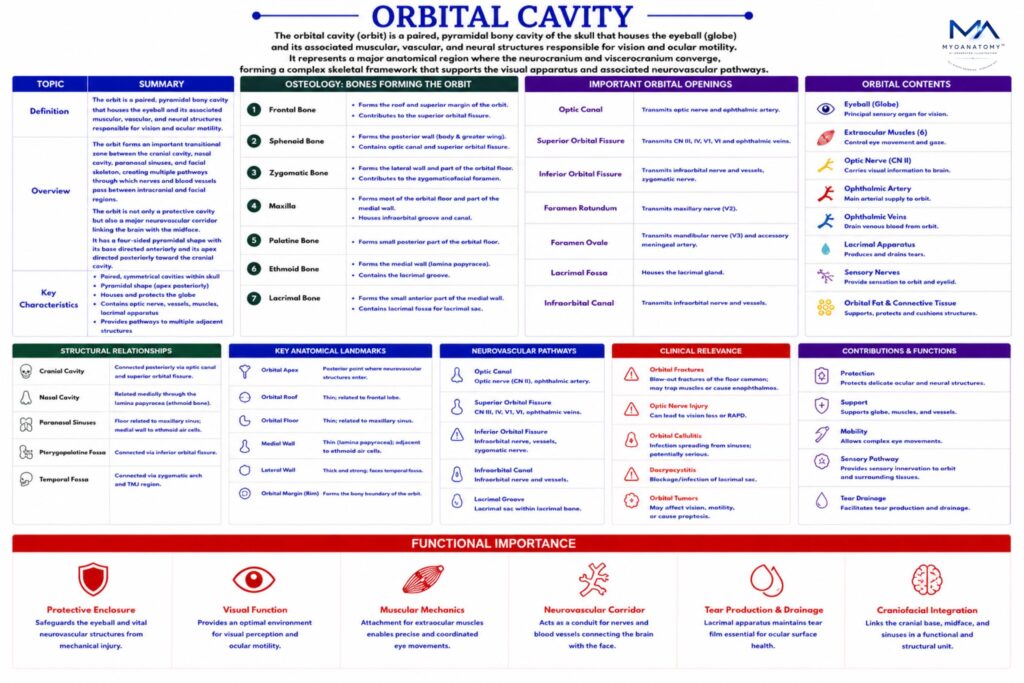
Anatomically, the orbit forms an important transitional zone between the cranial cavity, nasal cavity, paranasal sinuses, and facial skeleton, creating multiple pathways through which nerves and blood vessels pass between intracranial and facial regions.
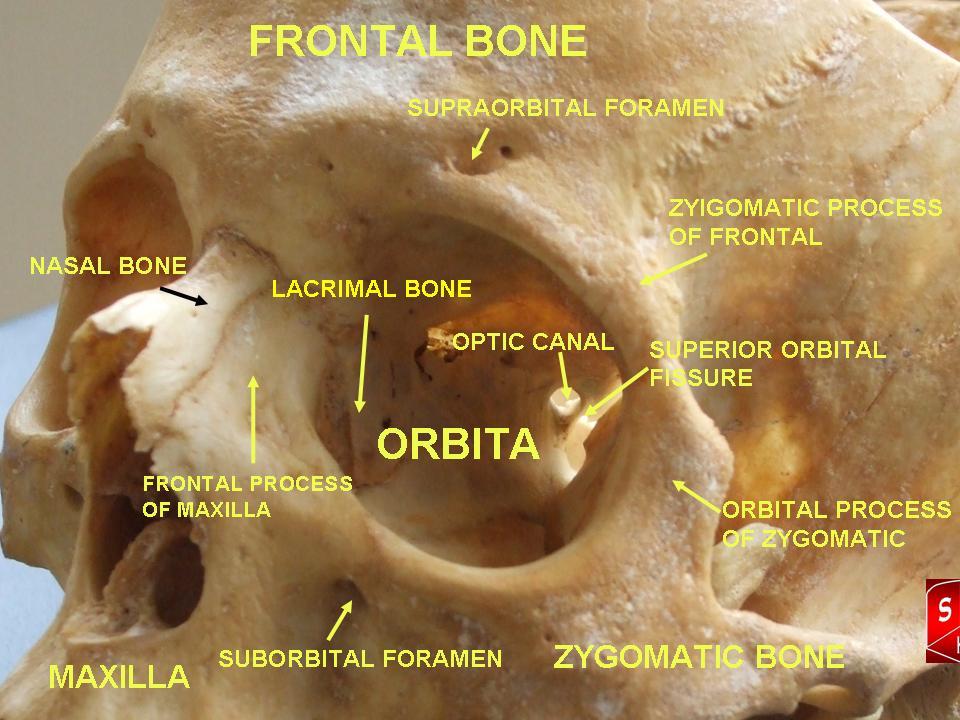
The orbit therefore represents not only a protective cavity for the eye, but also a major neurovascular corridor linking the brain with the midface.
The orbit has a four-sided pyramidal shape, with its base directed anteriorly and its apex directed posteriorly toward the cranial cavity.