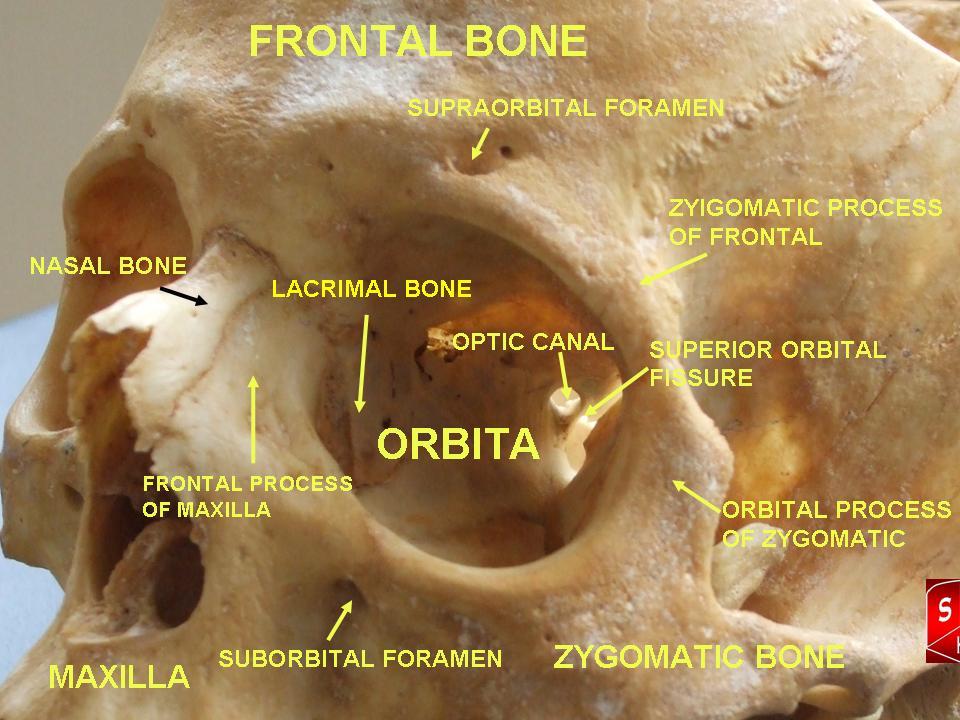
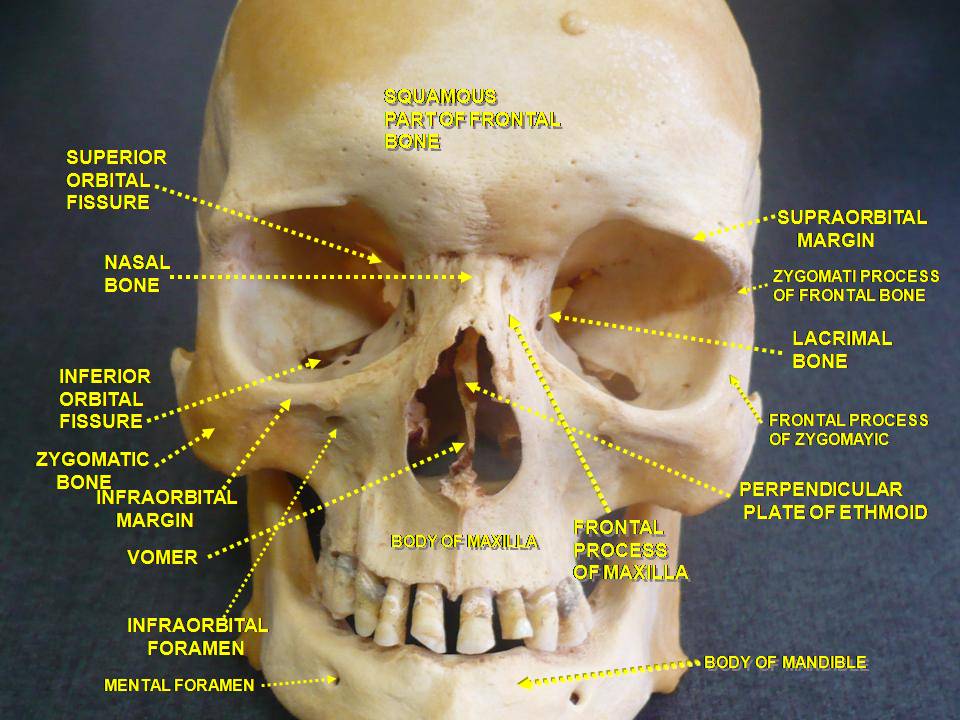
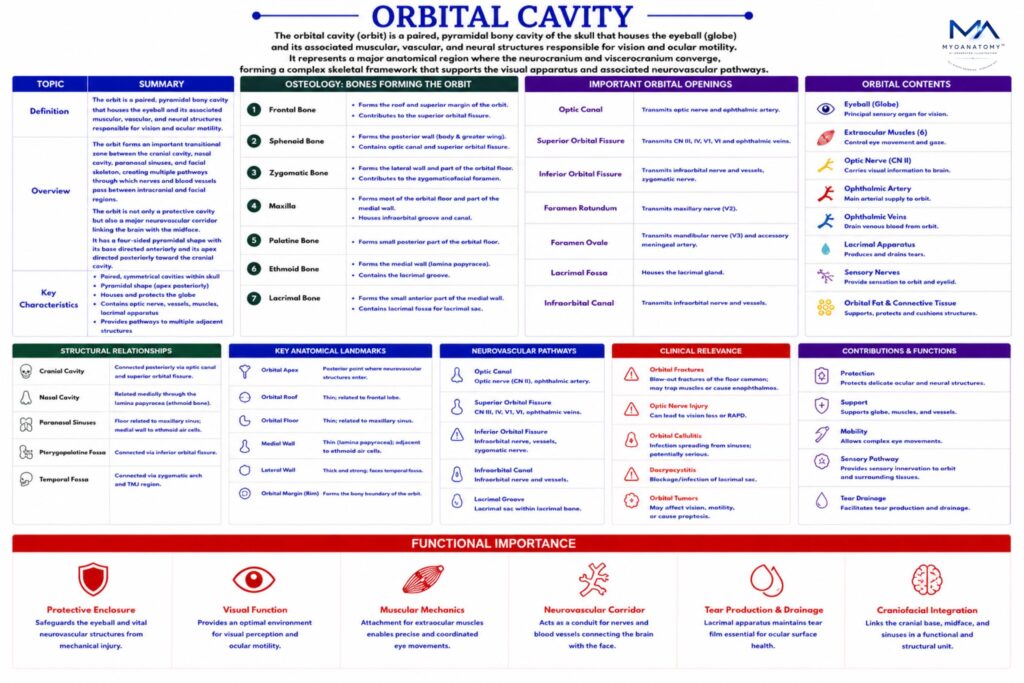
A slit-like opening between the greater and lesser wings of the sphenoid, connecting the orbit with the middle cranial fossa.
Transmits:
oculomotor nerve (CN III)
trochlear nerve (CN IV)
abducens nerve (CN VI)
ophthalmic nerve (CN V1: lacrimal, frontal, nasociliary branches)
superior ophthalmic vein
Functional significance:
controls extraocular movement and orbital sensation.
Clinical relevance:
lesions → ophthalmoplegia, ptosis, sensory loss (V1).