Orbital Cavity
MYO CORE
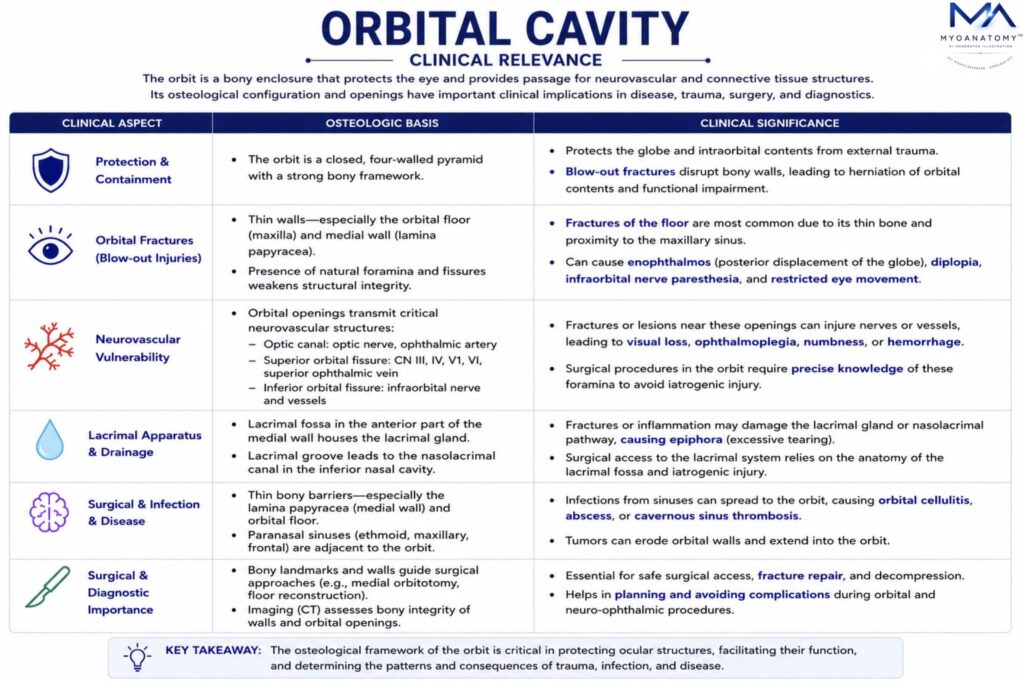
Clinical Relevance
The orbit is a region of major clinical importance because it forms a confined osteofascial compartment containing the globe, extra-ocular muscles, optic nerve, ophthalmic vessels, cranial nerves, fascial sheaths, and the lacrimal apparatus, while maintaining close anatomical continuity with the cranial cavity, paranasal sinuses, nasal cavity, pterygopalatine region, and facial skeleton.
OVERVIEW
Its clinical relevance therefore derives not only from ocular function itself, but from the fact that orbital disease may reflect or transmit pathology involving adjacent intracranial, sinonasal, vascular, neurological, and maxillofacial structures.
Because the orbit is rigidly bounded by bone except at its anterior opening, pathological processes such as haemorrhage, oedema, tumour expansion, or infection may rapidly increase intraorbital pressure. This may compromise venous drainage, restrict ocular motility, displace the globe, and, most importantly, threaten the optic nerve and its vascular supply. For this reason, many orbital disorders are not merely local eye conditions, but potential vision-threatening or even life-threatening emergencies
ANATOMY
Orbital Fractures
Orbital trauma most commonly affects the orbital floor and medial wall, which are structurally thin and therefore mechanically vulnerable. A blow-out fracture classically follows blunt trauma to the orbital region, producing a sudden increase in intraorbital pressure that is transmitted to these weak walls. The floor may fracture into the maxillary sinus, while the medial wall may fail into the ethmoidal air cells.
The clinical importance of such fractures lies in both skeletal disruption and soft-tissue entrapment. Herniation of orbital fat and incarceration of the inferior rectus or adjacent soft tissues may restrict ocular elevation and produce diplopia, especially on upward gaze. Injury to the infraorbital nerve within the infraorbital groove and canal may cause sensory loss or paraesthesia over the lower eyelid, cheek, upper lip, and lateral nose. Posterior displacement of the globe may result in enophthalmos, particularly when orbital volume increases because of floor collapse.
Thus, orbital fracture is not simply a fracture of bone; it is a lesion that may affect ocular alignment, sensory innervation, globe position, and facial symmetry simultaneously.
Orbital Apex Lesions
The orbital apex is one of the most clinically critical regions of the orbit because it represents the point of convergence of the optic canal and superior orbital fissure. Structures traversing this region include the optic nerve, ophthalmic artery, oculomotor nerve, trochlear nerve, abducens nerve, and branches of the ophthalmic division of the trigeminal nerve.
A lesion at the orbital apex, whether due to inflammation, neoplasm, trauma, haemorrhage, or invasive infection, may therefore produce a combined neuro-ophthalmic syndrome. Typical manifestations include visual loss from optic nerve involvement, ophthalmoplegia from paralysis of extra-ocular muscle innervation, ptosis from oculomotor dysfunction, fixed or poorly reactive pupil when parasympathetic fibres are affected, and sensory loss in the forehead, upper eyelid, and cornea through involvement of the ophthalmic nerve.
This region is clinically important because a relatively small lesion may produce severe functional deficit owing to the extreme anatomical concentration of neurovascular structures within a narrow space.
Superior Orbital Fissure
The superior orbital fissure provides communication between the middle cranial fossa and the orbit and transmits cranial nerves III, IV, VI, and V1, together with the superior ophthalmic vein. Pathology at this fissure may therefore produce a pattern resembling orbital apex disease but without primary optic nerve involvement unless the lesion extends medially into the optic canal.
Clinically, superior orbital fissure syndrome may present with ophthalmoplegia, ptosis, dilated pupil, impaired corneal sensation, and venous congestion. The distinction between orbital apex syndrome and isolated superior orbital fissure involvement is anatomically important because direct optic nerve compromise strongly suggests more medial or apical extension.
Infections Spread
The orbit is especially vulnerable to spread of infection from the paranasal sinuses, most commonly from the ethmoidal sinuses, because the medial orbital wall contains the lamina papyracea, an extremely thin osseous plate. Infection may spread directly through this wall or through valveless venous channels.
This anatomical relationship explains the frequency and seriousness of orbital cellulitis. Once infection extends into the orbit proper, the patient may develop painful eye movement, eyelid swelling, proptosis, chemosis, reduced ocular motility, and visual disturbance. Because the orbit is a closed space, inflammatory swelling may increase pressure around the optic nerve and central retinal vessels, placing vision at risk.
The clinical significance is therefore profound: what begins as sinus disease may progress into a vision-threatening orbital infection and, in severe cases, may extend further into intracranial venous channels.
Cavernous Sinus
The venous drainage of the orbit is of major clinical importance because the superior and inferior ophthalmic veins communicate with the cavernous sinus, and these veins are valveless. This permits bidirectional spread of infection or thrombosis.
As a result, infections of the orbit, nasal region, or medial facial region may spread to the cavernous sinus, producing cavernous sinus thrombosis. Because the cavernous sinus is closely related to cranial nerves III, IV, V1, V2, and VI, as well as the internal carotid artery, involvement may produce ophthalmoplegia, facial sensory deficit, venous congestion, chemosis, proptosis, severe headache, and systemic toxicity.
The anatomical basis of this complication makes the orbit a key gateway between superficial facial infection and intracranial disease.
Extraocular Muscle
The orbit contains the extra-ocular muscles in a precisely arranged biomechanical system that allows coordinated binocular gaze. Any condition that alters their innervation, mechanical freedom, or anatomical alignment may produce diplopia.
Diplopia may therefore arise from cranial nerve palsy, muscular inflammation, entrapment after fracture, displacement of the globe, or pathological restriction within the orbit. This makes disturbed eye movement one of the most useful clinical indicators that orbital disease is affecting either the muscular apparatus itself or the nerves that control it.
Lacrimal Drainage
The lacrimal gland occupies the superolateral part of the orbit within the lacrimal fossa of the frontal bone. Enlargement due to inflammation or neoplasm may produce inferomedial displacement of the globe, fullness of the upper lateral eyelid, and ocular discomfort.
This is clinically important because the direction of globe displacement often reflects the anatomical site of the lesion within the orbit and may therefore guide diagnosis before imaging.
Surgical Importance
The orbit is of major importance in ophthalmic, maxillofacial, ENT, and neurosurgical practice. Surgical intervention requires precise knowledge of orbital walls, fissures, canals, neurovascular pathways, and fascial planes in order to avoid visual loss, haemorrhage, or cranial nerve injury. Similarly, radiological interpretation of fractures, masses, sinus spread, and apical lesions depends on a detailed anatomical understanding of orbital compartments and communications.
For this reason, orbital anatomy is not only descriptive anatomy; it is directly applied anatomy essential to trauma care, infection management, neuro-ophthalmology, skull base surgery, and craniofacial reconstruction
SUMMARY TABLE