
Sacral Plexus
The sacral plexus is a fusion of the ventral rami of the spinal nerves L4–S4 (via the lumbosacral trunk), organized on the posterolateral pelvic wall anterior to piriformis,
Within this deep pelvic compartment, fibers converge toward the greater sciatic foramen, where major branches – predominantly the sciatic nerve – exit inferior to piriformis, establishing continuity with the gluteal region and posterior lower limb.
The sciatic nerve (L4–S3), representing the principal composite output, divides into tibial and common fibular components, coordinating hip extension, knee flexion, and distal limb motor and sensory control.
Functionally, the plexus integrates GSE, GSA, and postganglionic sympathetic fibers, enabling high-level coordination of locomotion, stance stability, and dynamic postural regulation through multisegmental neural convergence.
Clinically, its deep pelvic location predisposes it to compression or injury (e.g., piriformis syndrome, pelvic trauma), producing characteristic sciatic-pattern deficits – posterior limb weakness, foot drop, and sensory loss
DESCRIPTION
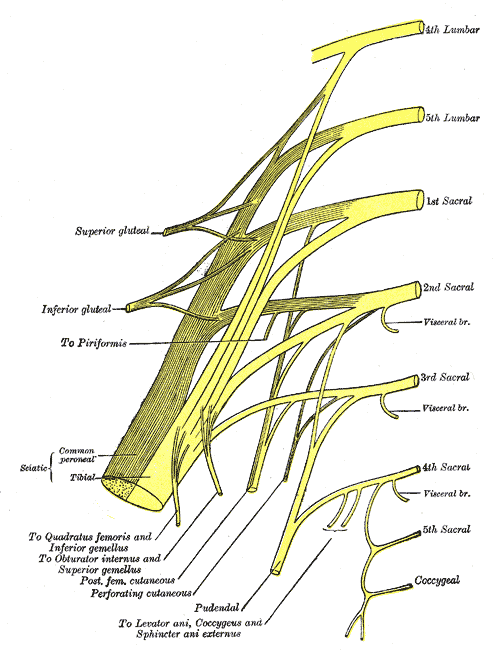
Plan of sacral and pudendal plexuses (Gray828)” – Henry Vandyke Carter, Gray’s Anatomy: Anatomy of the Human Body. Source: Wikimedia Commons. Public Domain.
AI-Generated Illustration-MyoAnatomy
Description
AI-Generated Illustration-MyoAntomy
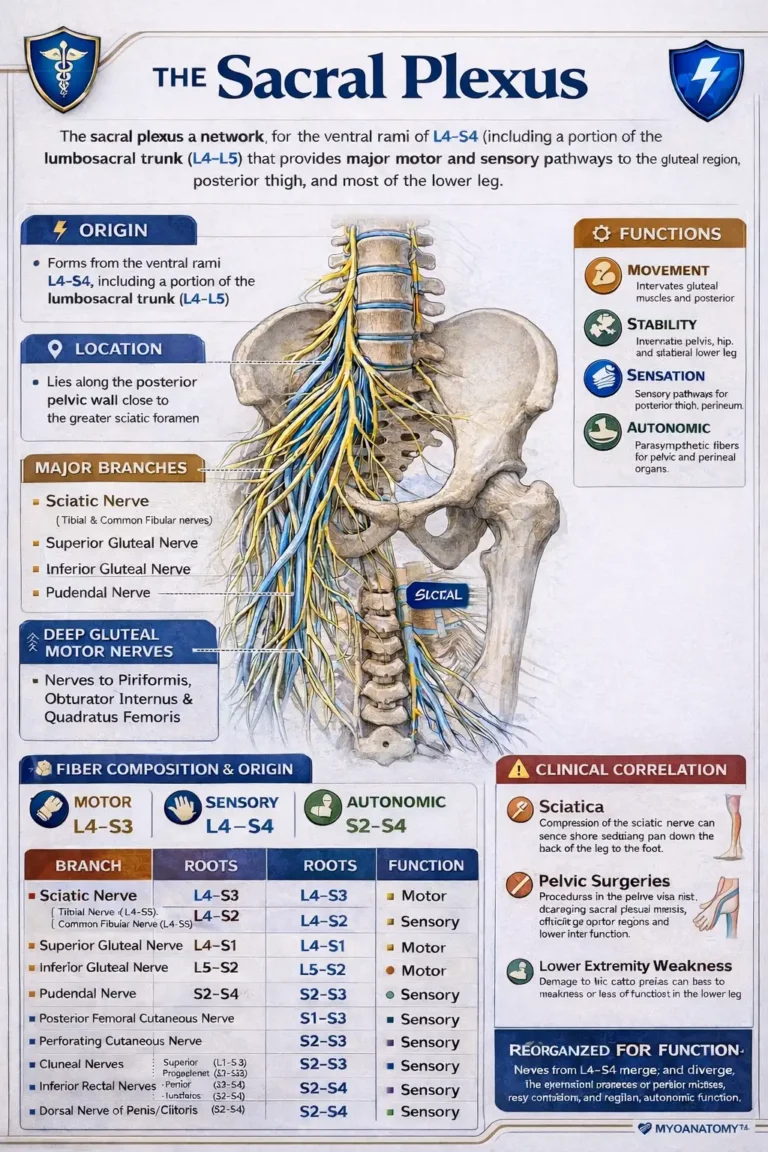
The sacral plexus is a fusion of the ventral rami of the spinal nerves (L4–S4) formed by the lumbosacral trunk (L4–L5) and ventral rami of S1–S4, organized on the pelvic (anterior) surface of piriformis along the posterior pelvic wall. Within this confined space, fibers undergo division into anterior (flexor–adductor) and posterior (extensor–abductor) components followed by recombination into large terminal branches that exit the pelvis via the greater sciatic foramen, predominantly inferior to piriformis, establishing the principal neural outflow to the gluteal region and lower limb.
The sciatic nerve (L4–S3) represents the dominant continuation, containing tibial (anterior division) and common fibular (posterior division) components that remain functionally distinct, distributing motor and sensory supply to all compartments of the leg and foot.
Proximal branches include the superior gluteal nerve (L4–S1) for pelvic stabilization, inferior gluteal nerve (L5–S2) for hip extension, posterior femoral cutaneous nerve (S1–S3) for posterior thigh sensation, and pudendal nerve (S2–S4) for perineal somatic function.
Each branch carries mixed GSE, GSA, and postganglionic sympathetic fibers, enabling integrated motor output, somatosensory feedback, and autonomic regulation.
Functionally, the plexus serves as the primary neuromechanical axis of the posterior chain, coordinating hip extension, knee flexion, and distal limb control for gait and postural stability.
Clinically, sacral plexus lesions produce a plexopathy pattern – multisegmental, non-dermatomal deficits with combined motor and sensory involvement (e.g., posterior limb weakness, foot drop), distinguishing them from isolated root or peripheral nerve injuries.
Exam Question
Explain how division and recombination within the sacral plexus (L4–S4) enable multisegmental integration of GSE, GSA, and GVE fibers, and analyze how this organization forms the sciatic nerve as a composite conduit for posterior chain control, distinguishing the clinical pattern of plexopathy from radiculopathy and peripheral nerve lesions.
MOTOR BRANCHES
Gluteal Nerves
The gluteal nerves are motor branches of the sacral plexus (L4–S2) derived from posterior divisions and supply the intrinsic musculature of the gluteal region, forming the principal neural system for pelvic stabilization and hip extension mechanics.
They exit the pelvis via the greater sciatic foramen in relation to piriformis, reflecting precise functional topography.
The superior gluteal nerve (L4–S1) passes superior to piriformis and supplies gluteus medius, gluteus minimus, and tensor fasciae latae, constituting the primary abductor – stabilizing pathway that maintains pelvic equilibrium during single-limb stance.
The inferior gluteal nerve (L5–S2) passes inferior to piriformis and supplies gluteus maximus, forming the principal extensor pathway responsible for powerful hip extension during propulsion.
Both nerves carry GSE fibers exclusively, consistent with their derivation from the dorsal muscle mass, and together integrate stabilization and propulsion within the posterior kinetic chain.
Clinically, superior gluteal nerve injury results in Trendelenburg gait due to loss of pelvic stabilization, while inferior gluteal nerve injury produces weak hip extension, impairing forceful movements such as rising and climbing.
Exam Question
Explain how the posterior-division origin of the gluteal nerves determines their motor specialization, and analyze how the superior and inferior gluteal nerves coordinate pelvic stabilization and hip extension during gait.
Deep Gluteal Motor Nerves
The nerves to piriformis, obturator internus, and quadratus femoris are short motor branches of the sacral plexus (L4–S2) arising from anterior divisions, supplying the deep lateral rotator group of the hip, derived from the ventral muscle mass. These nerves course through the greater and lesser sciatic foramina, forming a compact neurofunctional system positioned around the posterior aspect of the hip joint.
The nerve to piriformis (S1–S2), nerve to obturator internus (L5–S2), and nerve to quadratus femoris (L4–S1) innervate muscles that act collectively as a deep stabilizing complex, producing lateral rotation and dynamic compression of the femoral head into the acetabulum.
All carry GSE fibers and operate as fine-tuning stabilizers of the hip, analogous to a rotator cuff system, maintaining posterior hip stability and preventing shear forces during dynamic activity.
Functionally, they regulate rotational alignment and joint congruency, particularly during stance phase and load transfer, rather than generating large-scale movement.
Clinically, dysfunction contributes to deep gluteal syndrome, impaired rotational control, and posterior hip instability, affecting gait precision despite preserved gross motor strength
Exam Question
Explain how the anterior-division origin of the deep gluteal motor nerves reflects their derivation from ventral muscle mass, and analyze how their coordinated activity stabilizes the femoral head and regulates rotational alignment during load-bearing movement.
Sciatic Nerve
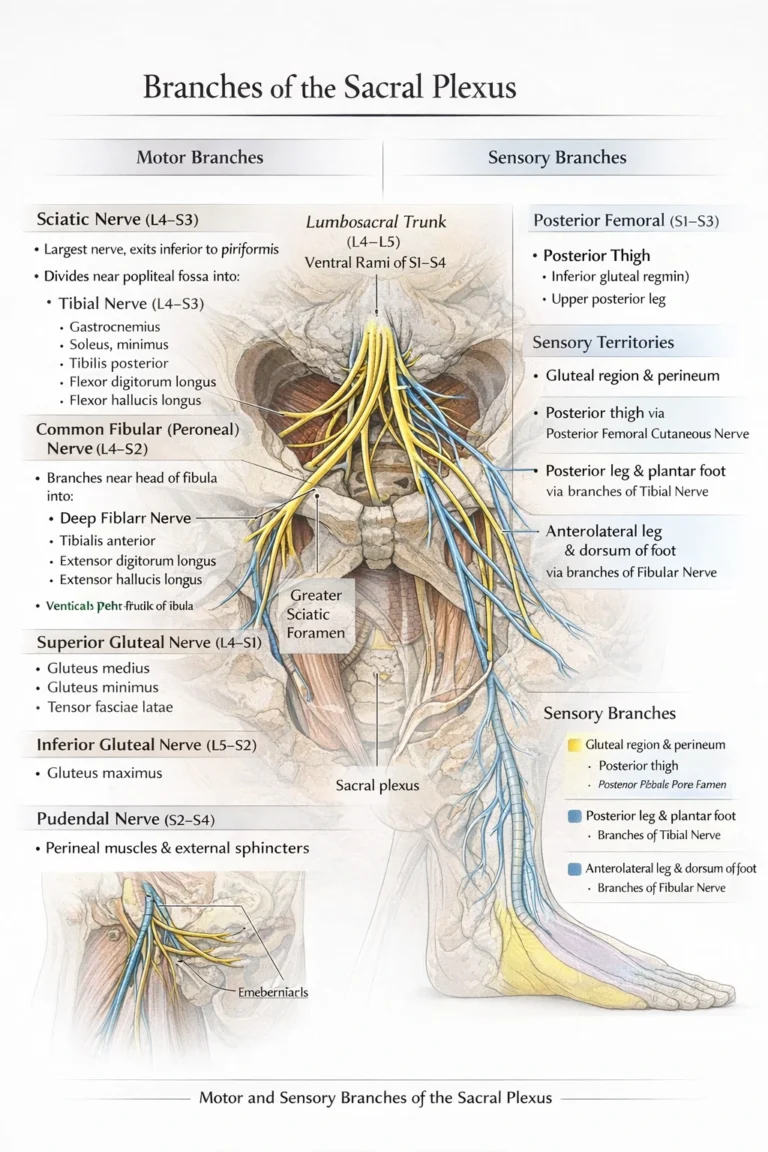
The sciatic nerve is the principal terminal branch of the sacral plexus (L4–S3), formed by the convergence of anterior and posterior divisions into a composite nerve containing functionally distinct tibial (anterior divisions) and common fibular (posterior divisions) components.
It exits the pelvis via the greater sciatic foramen inferior to piriformis, courses deep to gluteus maximus, and descends along the posterior thigh before dividing into its terminal branches.
Structurally, it functions as a multisegmental integrative conduit, in which fibers remain partially segregated within a common sheath. It carries GSE fibers to the posterior thigh and all compartments of the leg and foot, GSA fibers for extensive cutaneous and proprioceptive input, and postganglionic sympathetic (GVE) fibers for vascular regulation.
Topographically, sciatic nerve exits inferiro to the piriformis, courses deep to gluteus Maximus muscle over the posterior hip rotators, and descends along adductor magnus in the posterior thigh dividing into the tibial nerve and common fibular nerves near the popliteal fossa.
Functionally, it forms the central axis of the posterior kinetic chain, coordinating knee flexion and all distal limb movements, while linking proximal stability with distal precision during gait. Its dual-division architecture preserves functional separation of flexor–adductor and extensor–abductor systems within a single pathway.
Clinically, sciatic nerve lesions produce multicompartemental deficits, including posterior thigh weakness, loss of knee flexion, and distal motor impairment such as foot drop or loss of plantarflexion, with widespread sensory loss below the knee, reflecting disruption of a composite, multisegmental system.
Exam Question
Explain how the composite organization of the sciatic nerve enables functional segregation within a single conduit, and analyze how this underlies posterior chain biomechanics and the differential clinical patterns of tibial versus common fibular involvement.
Common Fibular Nerve
The common fibular nerve is the lateral terminal division of the sciatic nerve (L4–S2), derived from posterior divisions of the sacral plexus, and supplies the anterior and lateral compartments of the leg.
It separates from the tibial component in the distal thigh or popliteal fossa, courses laterally along the tendon of biceps femoris, and winds superficially around the neck of the fibula, where it is subcutaneous and highly vulnerable, before dividing into its terminal branches:
the deep fibular and superficial fibular nerves. Proximally, it also supplies the short head of biceps femoris.
Structurally, it represents a continuation of posterior division fibers maintaining functional specificity for the extensor – dorsiflexor and abductor – evertor systems, while carrying integrated GSE, GSA, and postganglionic sympathetic (GVE) components.
The deep fibular nerve supplies the anterior compartment (dorsiflexors and toe extensors) and provides sensory innervation to the first dorsal web space, while:
Superficial fibular nerve supplies the lateral compartment (evertors) and provides cutaneous innervation to the anterolateral leg and most of the dorsum of the foot.
Topographically, its superficial course around the fibular neck makes it particularly susceptible to compression, trauma, and external pressure, explaining its high clinical vulnerability.
Functionally, the nerve is essential for dorsiflexion, toe extension, and foot eversion, forming a critical component of the swing phase of gait, where it ensures foot clearance and prevents toe drag. Its activity balances the plantarflexor system, maintaining coordinated ankle mechanics and dynamic stability.
Clinically, injury results in foot drop, characterized by loss of dorsiflexion and toe extension with preserved plantarflexion, accompanied by sensory loss over the anterolateral leg and dorsum of the foot (sparing the first web space if superficial branch isolated).
Exam Question
Explain how the posterior-division origin of the common fibular nerve determines its specialization for the extensor–dorsiflexor system, and analyze how its anatomical course around the fibular neck accounts for the characteristic motor and sensory deficits observed in foot drop..
Tibial Nerve
The tibial nerve is the larger terminal branch of the sciatic nerve, derived from the anterior divisions of L4–S3, and represents the principal motor and sensory pathway of the posterior compartment of the leg and plantar aspect of the foot. It carries GSE, GSA, and postganglionic sympathetic (GVE) fibers, maintaining functional continuity with the flexor–plantar system of the lower limb.
Topographically – the tibial nerve separates from the sciatic nerve typically at the superior angle of the popliteal fossa and descends vertically through the fossa, lying superficial to the popliteal vessels and deep to the fascial roof. It continues inferiorly beneath the tendinous arch of soleus, coursing within the deep posterior compartment along the posterior tibial vessels. At the level posterior to the medial malleolus, it passes through the tarsal tunnel deep to the flexor retinaculum, where it divides into its terminal branches: the medial and lateral plantar nerves.
Structurally – the nerve functions as a highly organized somatic conduit, preserving anterior division fiber specialization for flexor and plantar musculature. It conveys GSE fibers to muscles of the posterior leg and intrinsic foot, GSA fibers for cutaneous innervation of the heel and sole, and sympathetic fibers regulating vascular tone within distal soft tissues.
Functionally – the tibial nerve is essential for plantarflexion, inversion, and toe flexion, forming the central effector pathway of the posterior kinetic chain during stance and propulsion. It enables push-off in gait, stabilizes the ankle joint, and coordinates intrinsic foot musculature necessary for fine postural adjustments. Its sensory component provides plantar feedback critical for balance and load distribution.
Clinically – injury to the tibial nerve results in loss of plantarflexion and toe flexion, weakened inversion, and inability to stand on the toes, producing a characteristic dorsiflexed and everted foot posture. Sensory loss involves the sole of the foot, often accompanied by neuropathic pain in cases of tarsal tunnel syndrome, where compression beneath the flexor retinaculum leads to paresthesia and motor weakness. Lesions proximal to the popliteal fossa produce more extensive deficits involving the posterior leg and plantar foot.
Exam Question
Explain how injury to the tibial nerve affects lower limb function, with reference to its root origin, anatomical course through the popliteal fossa and tarsal tunnel, and its motor, sensory, and autonomic distributions, and correlate these with the resulting deficits in gait and plantar function.
Pudendal Nerve
The pudendal nerve is a mixed somatic nerve arising from the ventral rami of S2–S4, representing the principal neural pathway of the perineum. It carries general somatic efferent (GSE), general somatic afferent (GSA), and postganglionic sympathetic (GVE) fibers, providing motor innervation to the external sphincters and perineal musculature, together with sensory supply to the external genitalia and perineal skin.
Topographically, the nerve exits the pelvis through the greater sciatic foramen inferior to piriformis, curves around the ischial spine and sacrospinous ligament, and re-enters the perineum via the lesser sciatic foramen. It then courses anteriorly within the pudendal (Alcock’s) canal along the lateral wall of the ischioanal fossa, accompanied by the internal pudendal vessels, before dividing into its terminal branches.
Structurally, it functions as a highly specialized somatic conduit, in which motor and sensory fibers remain organized for precise control of sphincteric and perineal function. It conveys GSE fibers to the external urethral and anal sphincters and perineal muscles, GSA fibers for discriminative and nociceptive sensation of the perineum and external genitalia, and sympathetic fibers that regulate vascular tone within erectile tissues.
Functionally, the pudendal nerve is essential for voluntary continence, providing active control over urination and defecation through coordinated contraction of the external sphincters. It contributes to pelvic floor stability via innervation of perineal musculature and supports sexual function through sensory input and autonomic modulation of genital vascular dynamics.
Clinically, pudendal nerve injury or entrapment, most commonly at the ischial spine or within Alcock’s canal, produces perineal pain, sensory deficits, and sphincter dysfunction, leading to urinary or fecal incontinence. It is particularly vulnerable in obstetric trauma and prolonged perineal compression. Targeted pudendal nerve block at the level of the ischial spine is a well-established technique for achieving perineal anesthesia in obstetric and surgical settings.
Exam Question
Explain how injury to the pudendal nerve results in loss of voluntary continence and altered perineal sensation, with reference to its root origin, anatomical course, and functional distribution.
SENSORY BRANCHES
Posterior Femoral Cutaneous Nerves
The gluteal nerves are motor branches of the sacral plexus (L4–S2) derived from posterior divisions and supply the intrinsic musculature of the gluteal region, forming the principal neural system for pelvic stabilization and hip extension mechanics.
They exit the pelvis via the greater sciatic foramen in relation to piriformis, reflecting precise functional topography.
The superior gluteal nerve (L4–S1) passes superior to piriformis and supplies gluteus medius, gluteus minimus, and tensor fasciae latae, constituting the primary abductor – stabilizing pathway that maintains pelvic equilibrium during single-limb stance.
The inferior gluteal nerve (L5–S2) passes inferior to piriformis and supplies gluteus maximus, forming the principal extensor pathway responsible for powerful hip extension during propulsion.
Both nerves carry GSE fibers exclusively, consistent with their derivation from the dorsal muscle mass, and together integrate stabilization and propulsion within the posterior kinetic chain.
Clinically, superior gluteal nerve injury results in Trendelenburg gait due to loss of pelvic stabilization, while inferior gluteal nerve injury produces weak hip extension, impairing forceful movements such as rising and climbing.
Exam Question
Explain how the posterior-division origin of the gluteal nerves determines their motor specialization, and analyze how the superior and inferior gluteal nerves coordinate pelvic stabilization and hip extension during gait.
Perforating Cutaneous Nerves
The nerves to piriformis, obturator internus, and quadratus femoris are short motor branches of the sacral plexus (L4–S2) arising from anterior divisions, supplying the deep lateral rotator group of the hip, derived from the ventral muscle mass. These nerves course through the greater and lesser sciatic foramina, forming a compact neurofunctional system positioned around the posterior aspect of the hip joint.
The nerve to piriformis (S1–S2), nerve to obturator internus (L5–S2), and nerve to quadratus femoris (L4–S1) innervate muscles that act collectively as a deep stabilizing complex, producing lateral rotation and dynamic compression of the femoral head into the acetabulum.
All carry GSE fibers and operate as fine-tuning stabilizers of the hip, analogous to a rotator cuff system, maintaining posterior hip stability and preventing shear forces during dynamic activity.
Functionally, they regulate rotational alignment and joint congruency, particularly during stance phase and load transfer, rather than generating large-scale movement.
Clinically, dysfunction contributes to deep gluteal syndrome, impaired rotational control, and posterior hip instability, affecting gait precision despite preserved gross motor strength
Exam Question
Explain how the anterior-division origin of the deep gluteal motor nerves reflects their derivation from ventral muscle mass, and analyze how their coordinated activity stabilizes the femoral head and regulates rotational alignment during load-bearing movement.
Cluneal Nerves
The cluneal nerves are a group of purely cutaneous nerves supplying the skin of the gluteal region, comprising the superior, middle, and inferior cluneal nerves, derived respectively from the posterior rami of L1–L3, posterior rami of S1–S3, and the posterior femoral cutaneous nerve (S1–S3). They carry general somatic afferent (GSA) fibers with accompanying postganglionic sympathetic (GVE) components, providing segmental sensory innervation to the buttock.
Topographically – the superior cluneal nerves emerge from the posterior lumbar rami and cross the iliac crest to supply the superolateral gluteal region; the middle cluneal nerves arise from posterior sacral rami, pass through the posterior sacral foramina, and supply the medial gluteal region overlying the sacrum; the inferior cluneal nerves branch from the posterior femoral cutaneous nerve beneath the gluteus maximus, curving around its inferior border to innervate the inferior gluteal region (gluteal fold).
Structurally – they represent segmental cutaneous conduits conveying GSA fibers for tactile, nociceptive, and thermal sensation, with associated sympathetic fibers regulating cutaneous vasomotor and sudomotor activity across the gluteal integument.
Functionally – the cluneal nerves provide complete sensory coverage of the gluteal skin, contributing to protective sensation, pressure detection, and positional awareness, particularly during sitting and locomotion, without any motor component.
Clinically – lesions produce localized sensory disturbances confined to their respective territories, with no motor deficit, a key diagnostic feature. Entrapment of the superior cluneal nerves at the iliac crest is a recognized cause of lower back pain, while involvement of middle or inferior cluneal nerves may contribute to sacroiliac or gluteal pain syndromes, often mimicking deeper musculoskeletal pathology.
Exam Question
Explain the segmental origin and anatomical distribution of the cluneal nerves as a unified sensory system of the gluteal region, and correlate their purely cutaneous function with the localized pattern of sensory deficits observed in clinical entrapment syndromes
Posterior Scrotal/Labial Nerves
The posterior scrotal (male) and posterior labial (female) nerves are superficial sensory branches of the perineal nerve, itself a division of the pudendal nerve (S2–S4). They carry general somatic afferent (GSA) fibers with accompanying postganglionic sympathetic (GVE) components, supplying the posterior aspect of the external genitalia and adjacent perineal skin.
Topographically – these nerves arise within the pudendal (Alcock’s) canal, where the perineal nerve divides into superficial branches. They pass anteriorly and medially, emerging from the canal to course within the superficial perineal space, where they distribute to the posterior scrotum or labia majora, forming an anastomotic network with adjacent perineal nerves.
Structurally – they function as terminal cutaneous branches, conveying GSA fibers for fine touch, pain, and temperature sensation. Their associated sympathetic fibers regulate cutaneous vasomotor and sudomotor activity, contributing to the physiological responsiveness of the perineal integument.
Functionally – they provide sensory innervation to the posterior external genitalia and perineal region, contributing to protective sensation, tactile discrimination, and sexual sensory input, particularly in areas subjected to mechanical contact and pressure.
Clinically – injury to these nerves results in localized sensory loss or dysesthesia of the posterior scrotum or labia, without motor deficit. They may be affected in perineal trauma, surgical procedures, or pudendal nerve entrapment, and are relevant in regional anesthesia involving pudendal or perineal nerve blocks.
Exam Question
Explain the anatomical origin and distribution of the posterior scrotal (labial) nerves, and correlate their course within the pudendal canal and superficial perineal space with the localized sensory deficits observed following injury
Inferior Rectal Nerves
The inferior rectal nerves are mixed branches of the pudendal nerve (S2–S4), carrying general somatic afferent (GSA), general somatic efferent (GSE), and postganglionic sympathetic (GVE) fibers. They provide sensory innervation to the anal canal below the pectinate line and perianal skin, together with motor supply to the external anal sphincter.
Topographically – the nerves arise from the pudendal nerve within or near the pudendal (Alcock’s) canal, then pass medially across the ischioanal fossa, traversing the fat-filled space toward the anal canal. They pierce the fascia of the external anal sphincter to reach the perianal region and distal anal canal.
Structurally – they function as short mixed branches, conveying GSE fibers to the external anal sphincter for voluntary control, GSA fibers for somatic sensation (pain, temperature, touch) of the lower anal canal and surrounding skin, and sympathetic fibers contributing to vascular regulation.
Functionally – the inferior rectal nerves are essential for voluntary continence, enabling contraction of the external anal sphincter, and provide somatic sensory input critical for distinguishing noxious stimuli in the anal region. Their sensory component underlies the sharp, well-localized pain associated with lesions below the pectinate line.
Clinically – injury results in loss of voluntary control of defecation (fecal incontinence) and sensory loss in the perianal region, often accompanied by reduced anal tone. They are at risk in ischioanal fossa infections, perianal surgery, and pudendal nerve entrapment, and are targeted indirectly in pudendal nerve block procedures.
Exam Question
Explain the anatomical course and functional significance of the inferior rectal nerves, and correlate their mixed innervation with the loss of voluntary continence and altered somatic sensation observed in lesions below the pectinate line.
Dorsal Nerve of Penis/ Clitoris
The dorsal nerve of the penis (male) or clitoris (female) is the terminal sensory branch of the pudendal nerve (S2–S4), carrying predominantly general somatic afferent (GSA) fibers with accompanying postganglionic sympathetic (GVE) components. It provides principal sensory innervation to the dorsal aspect of the external genitalia, including the highly specialized sensory structures of the glans.
Topographically – the nerve arises in the deep perineal space as a terminal branch of the pudendal nerve, then courses anteriorly along the ischiopubic ramus, accompanying the internal pudendal vessels. It passes beneath the pubic symphysis and runs along the dorsum of the penis or clitoris, lying lateral to the deep dorsal vein and supplying branches to the shaft and glans.
Structurally – it functions as a high-fidelity sensory conduit, transmitting GSA fibers specialized for fine touch and nociception, particularly within the glans. Sympathetic fibers regulate vascular tone within erectile tissues, contributing to the neurovascular integration of sexual function.
Functionally – the nerve provides precise sensory input essential for tactile discrimination and sexual function, especially within the glans penis or clitoris. It plays a critical role in sensory feedback during sexual activity, forming part of reflex arcs involved in arousal and orgasm.
Clinically – injury results in loss or reduction of genital sensation, particularly affecting the glans, with potential impairment of sexual function. It may be affected in pelvic trauma, surgical procedures, or pudendal nerve entrapment, and is a target in selective nerve block techniques for genital procedures.
Exam Question
Explain the anatomical course and functional significance of the dorsal nerve of the penis (clitoris), and correlate its specialized sensory distribution with the effects of injury on genital sensation and sexual function
Plantar Nerves
The medial and lateral plantar nerves are the terminal branches of the tibial nerve (S2–S3), carrying general somatic afferent (GSA), general somatic efferent (GSE), and postganglionic sympathetic (GVE) fibers. They provide the principal sensory innervation to the plantar surface of the foot, together with motor supply to intrinsic foot musculature.
Topographically – they arise within the tarsal tunnel posterior to the medial malleolus, where the tibial nerve divides beneath the flexor retinaculum. The medial plantar nerve courses anteriorly between abductor hallucis and flexor digitorum brevis, while the lateral plantar nerve passes obliquely across the sole toward the lateral aspect, lying deep to flexor tendons.
Structurally – they function as terminal mixed branches, conveying GSA fibers from the plantar skin and digits, GSE fibers to intrinsic foot muscles, and sympathetic fibers regulating cutaneous and vascular dynamics.
Functionally – the medial plantar nerve supplies sensation to the medial three-and-a-half digits and medial sole, analogous to the median nerve in the hand, while the lateral plantar nerve supplies the lateral one-and-a-half digits and lateral sole, analogous to the ulnar nerve. Together, they provide critical sensory feedback for balance, pressure distribution, and gait mechanics.
Clinically- compression within the tarsal tunnel results in plantar pain, paresthesia, and sensory disturbance, known as tarsal tunnel syndrome. Injury leads to loss of plantar sensation and impaired intrinsic foot function, affecting gait stability and weight-bearing dynamics
Exam Question
Explain the anatomical course and functional distribution of the medial and lateral plantar nerves, and correlate their segmental sensory territories with the effects of tibial nerve compression within the tarsal tunnel.
FUNCTIONAL IMPORTANCE
Motor Control
The sacral plexus (L4–S4) constitutes the principal motor outflow to the posterior chain of the lower limb, predominantly via the sciatic nerve and its tibial and common fibular divisions. It orchestrates hip extension (gluteus maximus), knee flexion (hamstrings), and complex ankle–foot movements, including plantarflexion, dorsiflexion, inversion, and eversion.
Functionally, this system acts as the primary propulsive engine of locomotion, generating force for walking, running, and climbing. Simultaneously, it enables fine distal motor control, allowing precise modulation of foot position and ground interaction, essential for efficient gait and adaptive movement across variable terrain.
Pelvis Stabilization
Through the superior and inferior gluteal nerves, the sacral plexus innervates the gluteal musculature, particularly the gluteus medius and minimus, which are critical dynamic stabilizers of the pelvis. During single-leg stance, these muscles maintain horizontal pelvic alignment, preventing contralateral pelvic drop.
Functionally, this stabilization ensures efficient force transmission between trunk and lower limb, maintaining postural equilibrium, gait symmetry, and mechanical efficiency. Disruption leads to instability patterns such as Trendelenburg gait, reflecting failure of lateral pelvic support.
Sensory Integration
The sacral plexus provides extensive somatic sensory innervation to the posterior lower limb, gluteal region, perineum, and plantar foot, via branches such as the posterior femoral cutaneous, pudendal, and tibial nerves. These pathways transmit cutaneous sensation (touch, pain, temperature) and deep proprioceptive input from muscles, joints, and fascia.
Functionally, this afferent network enables continuous central integration of limb position, load distribution, and surface contact, forming the basis of balance, coordinated movement, and adaptive gait control. It is essential for real-time motor correction and prevention of instability.
Pelvic Floor Control
Via the pudendal nerve (S2–S4), the sacral plexus provides motor and sensory innervation to the pelvic floor musculature, including the external urethral and anal sphincters and associated perineal muscles. This system integrates voluntary somatic control with autonomic pelvic functions.
Functionally, it is essential for urinary and fecal continence, organ support, and reproductive function, enabling precise regulation of sphincter tone and coordinated pelvic activity. Disruption results in incontinence, pelvic instability, and impaired functional control of pelvic organs, reflecting loss of integrated neuromuscular regulation.
CLINICAL RELEVANCE
Sciatic Neuropathy
The most clinically significant pathology of the sacral plexus involves the sciatic nerve, which may be injured by pelvic trauma, hip dislocation, fractures, or compression (e.g., piriformis syndrome). As the sciatic nerve carries fibers to the majority of the lower limb, lesions produce combined deficits affecting the posterior thigh, leg, and foot.
Functionally, this results in loss of knee flexion, impairment of all distal movements, and widespread sensory deficits below the knee, reflecting disruption of both tibial and common fibular components. The integrated nature of the nerve leads to a global failure of lower limb motor coordination and load-bearing capacity, severely compromising locomotion.
Foot Drop
Selective injury to terminal branches of the sciatic nerve produces characteristic distal deficits. Damage to the common fibular nerve results in loss of dorsiflexion and toe extension, leading to foot drop, typically compensated by a high-stepping gait. In contrast, injury to the tibial nerve results in loss of plantarflexion and toe flexion, impairing the push-off phase of gait
Functionally, these deficits disrupt the critical phases of walking – foot clearance and propulsion -leading to inefficient, unstable, and energy-demanding gait patterns. This highlights the functional division of the sciatic nerve into extensor–dorsiflexor and flexor–plantar systems.
Pelvis Stabilization
Injury to the superior gluteal nerve compromises the function of gluteus medius and minimus, resulting in impaired pelvic stabilization during single-leg stance. This produces a Trendelenburg gait, characterized by contralateral pelvic drop during walking.
Functionally, this reflects failure of lateral pelvic support, leading to loss of gait symmetry, balance, and efficient force transmission between trunk and lower limb. It represents a disruption of proximal control mechanisms essential for stable locomotion.
Pudendal Nerve Disfucntion
Damage to the pudendal nerve (S2–S4) – commonly due to childbirth, pelvic trauma, or surgical injury – results in sensory loss in the perineum and dysfunction of pelvic floor musculature. This includes impairment of the external urethral and anal sphincters, leading to urinary and/or fecal incontinence.
Functionally, this highlights the role of the sacral plexus beyond locomotion, integrating somatic motor control with pelvic and visceral regulation. Loss of pudendal function disrupts continence, organ support, and coordinated pelvic activity, reflecting breakdown of a highly specialized neuromuscular system.