
Cervical Plexus
The cervical plexus is a segmentally derived, functionally integrated network formed by the anterior (ventral) rami of C1–C4, transforming discrete spinal input into coordinated cervical and upper thoracic output.
It lies deep to the sternocleidomastoid within the prevertebral fascia, adjacent to the carotid sheath and prevertebral muscles, forming a key interface between somatic, visceral, and vascular structures.
Structurally, it consists of interconnecting C1–C4 loops without trunks or cords, undergoing direct fascicular redistribution into superficial (cutaneous) and deep (motor) branches.
It carries mixed fibers: motor (GSE) to prevertebral and infrahyoid muscles (via ansa cervicalis) and diaphragm (phrenic nerve, C3–C5); sensory (GSA) to anterolateral neck, auricular, and supraclavicular skin; and autonomic (GVE) sympathetic fibers.
The phrenic nerve is the principal output linking cervical segments to respiration.
Clinically, root lesions cause dermatomal/myotomal deficits, plexus lesions cause mixed non-segmental dysfunction, and phrenic injury leads to diaphragmatic paralysis.
Functionally, it preserves segmental identity at roots but enables fiber recombination, producing multisegmental innervation, redundancy, and non-segmental clinical patterns.
BRANCHES
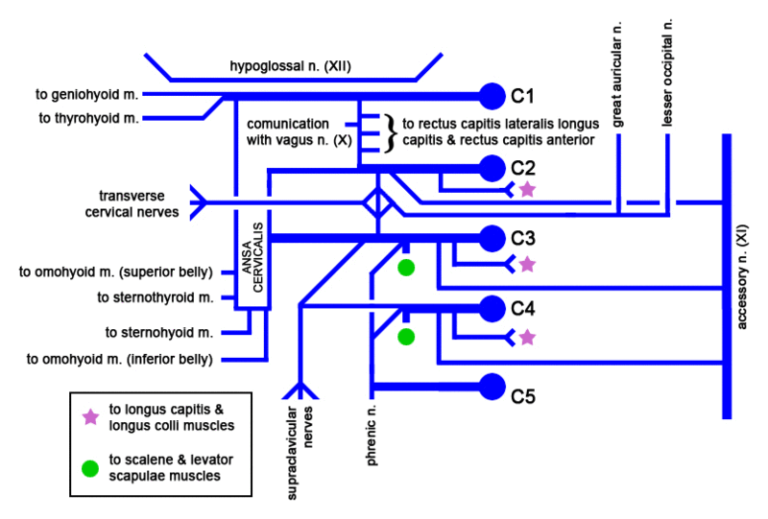
”Cervical Plexus”-Mikael Häggström via Wikimedia Commons. Public Domain
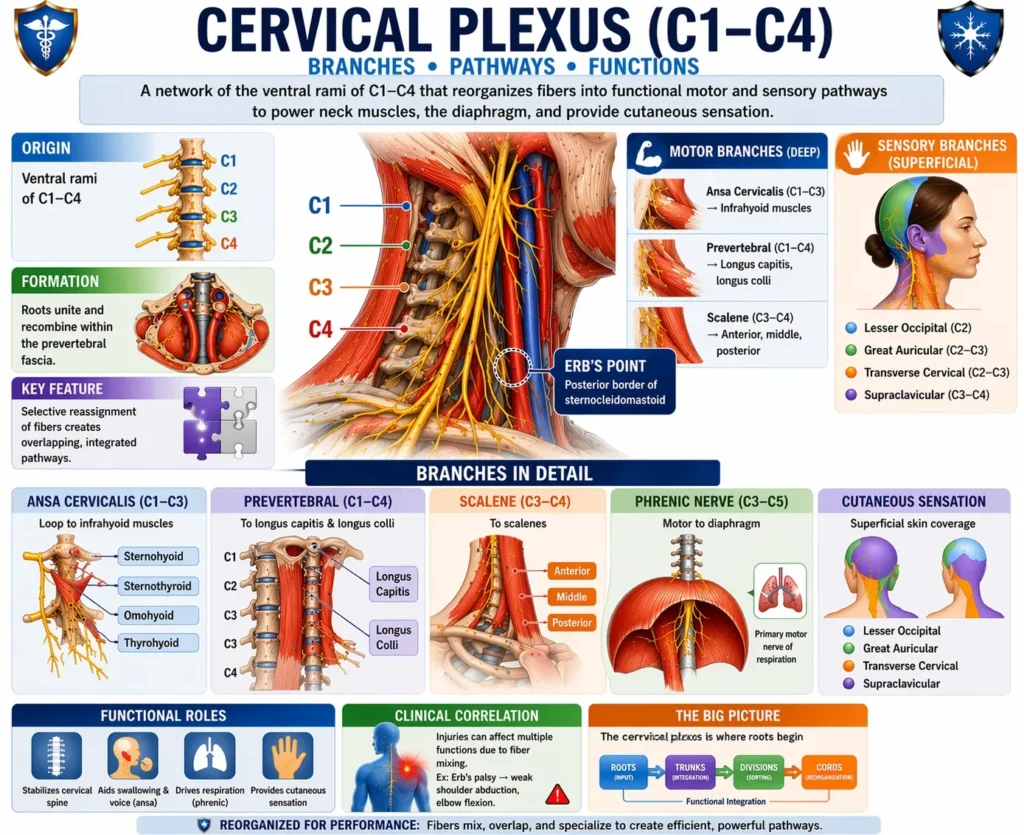
AI-Generated Illustration-MyoAnatomy
Description
AI-Generated Illustration-MyoAntomy
The cervical plexus (C1–C4) is a fusion of the ventral rami of the spinal nerves in which segmentally derived axons undergo progressive recombination and functional sorting within the prevertebral fascial compartment.
Initially, each root carries mixed fiber modalities – somatic motor (GSE), somatic sensory (GSA), and autonomic (GVE) – maintaining strict segmental identity; however, within the plexus, these fibers are selectively reassigned into composite peripheral pathways according to target tissue and functional demand rather than spinal origin.
Motor organization reflects task-oriented integration rather than segmental fidelity. Fibers from C1–C3 form the ansa cervicalis, coordinating infrahyoid musculature to regulate laryngeal positioning, airway patency, and swallowing biomechanics, while direct branches to prevertebral and scalene muscles stabilize the cervical spine and couple postural control with respiratory mechanics.
The phrenic nerve (C4) represents a critical longitudinal integration pathway, linking cervical spinal segments to thoracic function; it delivers rhythmically patterned motor output to the diaphragm and conveys visceral afferents from pleura, pericardium, and diaphragmatic peritoneum, forming a key substrate for referred pain and respiratory reflex arcs.
Sensory organization demonstrates topographic redistribution with partial preservation of segmental gradients. Cutaneous branches emerging at Erb’s point (punctum nervosum) disperse fibers from multiple roots via the lesser occipital, great auricular, transverse cervical, and supraclavicular nerves, producing overlapping sensory territories across the neck and upper thorax. This overlap reflects fascicular mixing within the plexus, ensuring continuity of sensation despite partial root compromise.
Functionally, the cervical plexus operates as a multisegmental integration hub, transforming discrete spinal inputs into coordinated neuromuscular outputs that align with biomechanical compartments (e.g., flexor vs postural systems) and physiological processes (e.g., ventilation, airway protection).
Clinically, this architecture explains the fundamental distinction between lesion patterns:
Root lesions produce precise dermatomal and myotomal deficits due to preserved segmental organization.
Plexus lesions result in non-segmental, composite deficits, reflecting disruption of already integrated fiber pools, often combining motor, sensory, and autonomic dysfunction across multiple territories.
Exam Question
“Explain the cervical plexus as a system of hierarchical neural redistribution, detailing the mechanisms by which segmental spinal inputs are reorganized into functionally integrated motor and sensory pathways, and critically relate this organization to the contrasting clinical patterns observed in radicular versus plexus lesions.”
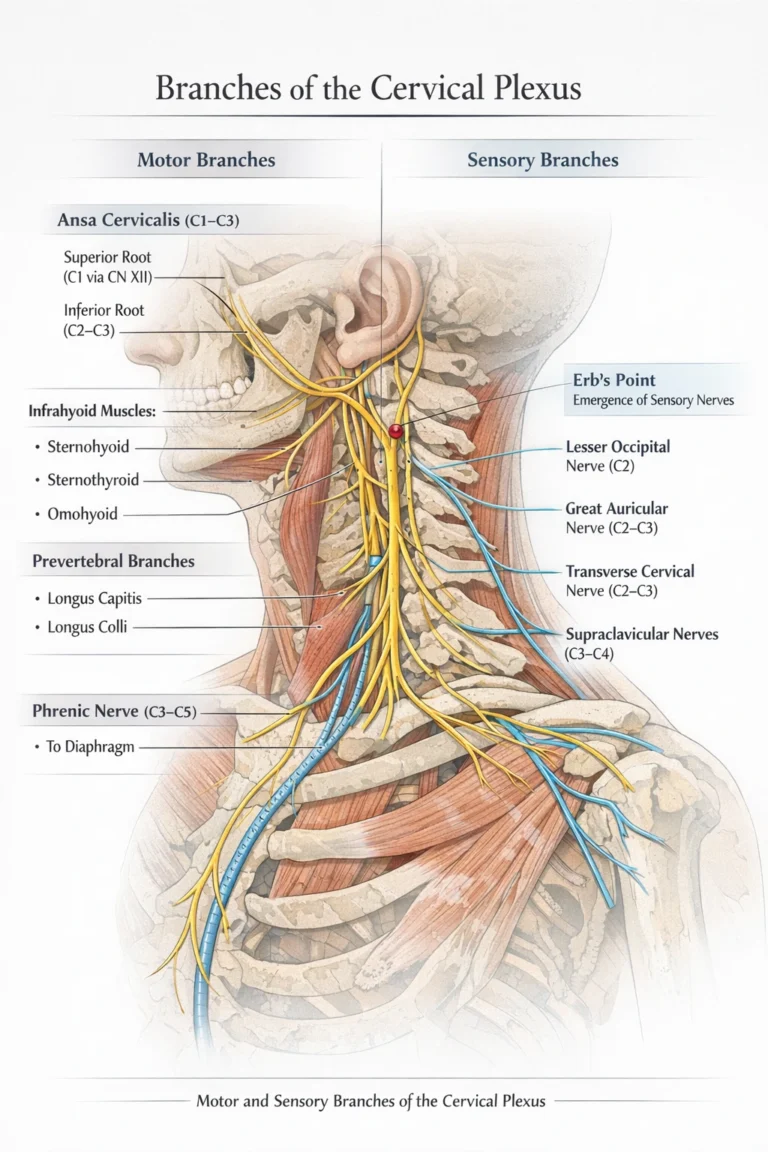
Motor Branches
The motor component of the cervical plexus (C1–C4) represents a functionally organized efferent system in which segmentally derived somatic motor fibers (GSE) are redistributed into coordinated pathways governing cervical stabilization, hyoid dynamics, and respiration.
Fibers are reorganized within the plexus into task-specific outputs that integrate multiple spinal levels into unified motor functions.
The ansa cervicalis (C1–C3) is a looped motor network formed by contributions from the upper cervical roots, with C1 fibers transiently traveling with the hypoglossal nerve (CN XII) before descending to join fibers from C2 and C3. This configuration enables redistribution of motor fibers to the infrahyoid musculature (sternohyoid, sternothyroid, omohyoid), which play a critical role in coordinated depression and stabilization of the hyoid bone.
Functionally, this system is essential for swallowing, phonation, and maintenance of airway patency, representing a mechanism by which segmental motor inputs are integrated into finely controlled laryngeal and cervical actions.
Exam Question
Critically evaluate cervical plexus motor organization as hierarchical redistribution, focusing on the ansa cervicalis, and explain how segmental motor fibers form coordinated pathways for hyoid movement, airway patency, and swallowing within cervical integration.”
Direct Muscular Branches
Direct muscular branches of the cervical plexus supply the prevertebral muscles, including longus capitis and longus colli, as well as contributing to the scalene musculature. These branches provide continuous segmental support for cervical spine stability and controlled flexion while functionally coupling postural control with respiratory mechanics, particularly through scalene-mediated elevation of the upper ribs during forced inspiration.
The phrenic nerve (C3-C5, primarily C4), arising with contributions from adjacent segments, constitutes the principal longitudinal motor pathway of the cervical plexus. It descends along the anterior surface of the anterior scalene muscle, enters the thoracic cavity, and provides the sole motor innervation to the diaphragm, thereby serving as the primary neural driver of ventilation. In addition, it conveys sensory afferents from the diaphragmatic pleura, pericardium, and central diaphragmatic peritoneum, forming the anatomical basis for referred pain patterns.
Functionally, the phrenic nerve exemplifies integration across anatomical regions, linking cervical spinal output to thoracic respiratory function and coordinating rhythmic motor activity essential for life.
Exam Question
“Analyze direct muscular branches of the cervical plexus as an interface of cervical stabilization and respiration, including prevertebral, scalene, and phrenic components, and explain their multisegmental and longitudinal integration.”
Sensory Branches
The sensory branches of the cervical plexus (C2–C4) form a functionally integrated cutaneous network in which segmentally derived somatic afferent fibers (GSA) undergo fascicular redistribution and recombination to supply overlapping peripheral territories of the neck, lower scalp, auricle, shoulder, and upper thoracic region.
These branches emerge at a common anatomical point along the posterior border of the sternocleidomastoid muscle, known clinically as Erb’s point, where fibers from multiple spinal levels converge and reorganize before dispersing superficially. Although their origin remains segmental, plexus-level integration disrupts strict dermatomal mapping, producing non-dermatomal, overlapping sensory fields characterized by redundancy.
This organization ensures preservation of sensation despite partial root injury and reflects a transition from segmental to regionally integrated sensory representation.
Functionally, the plexus transforms discrete spinal input into coordinated cutaneous perception across cervicothoracic regions, supporting integrated sensory feedback and adaptive resilience of afferent function.
Exam Question
Evaluate cervical plexus sensory organization as fascicular redistribution at Erb’s point, producing overlapping non-dermatomal fields and determining sensory preservation vs deficit in root and plexus lesions.”
Direct Sensory Branches
The direct sensory branches of the cervical plexus – the lesser occipital (C2), great auricular (C2–C3), transverse cervical (C2–C3), and supraclavicular nerves (C3–C4) – represent regionally organized outputs of redistributed segmental afferent fibers, arranged according to anatomical territory rather than strict spinal origin.
The lesser occipital nerve ascends along the posterior border of the sternocleidomastoid to supply the lateral occipital scalp and posterior auricular region, contributing to posterior cranial sensory continuity.
The great auricular nerve crosses superficially over the sternocleidomastoid toward the parotid region and external ear, supplying the parotid area, angle of the mandible, and auricle, and is clinically significant due to its vulnerability in surgical exposure.
The transverse cervical nerve courses horizontally across the neck to innervate the anterior cervical skin, providing integrated anterior sensory coverage.
The supraclavicular nerves descend inferiorly to supply the clavicular, shoulder, and upper thoracic regions, extending cervical afferent distribution caudally and demonstrating vertical integration across anatomical regions.
Collectively, these branches exemplify how plexus-level recombination transforms segmental sensory input into overlapping, functionally integrated cutaneous fields.
Exam Question
Analyze direct sensory branches as redistributed afferent pathways, where multisegmental and vertical integration create continuous cervicothoracic fields and non-segmental sensory loss.”
FUNCTIONAL IMPORTANCE
Respiratory Control
The cervical plexus exerts a critical role in respiratory physiology through the phrenic nerve (C3–C5), which provides the sole motor innervation to the diaphragm. This establishes the plexus as a direct neural interface between cervical spinal segments and thoracic ventilatory mechanics.
Diaphragmatic contraction generates negative intrathoracic pressure, enabling inspiration and sustaining ventilation.
Beyond simple motor output, this system integrates cervical spinal input with thoracic biomechanics, ensuring rhythmic, coordinated respiratory cycles.
Sensory afferents carried by the phrenic nerve from the pleura, pericardium, and diaphragm further contribute to reflexive modulation of respiration.
Thus, the cervical plexus represents a life-sustaining integrative pathway linking neural control to essential autonomic function.
Cervical Stability
Motor branches of the cervical plexus supply prevertebral muscles, scalene muscles, and infrahyoid musculature (via ansa cervicalis, C1–C3), forming a coordinated system for cervical spine stabilization and controlled movement.
Prevertebral muscles maintain segmental alignment and fine postural adjustments, while scalene muscles contribute to both stabilization and accessory respiratory function.
The infrahyoid muscles regulate hyoid positioning, which is essential for coordinated swallowing and airway patency.
Functionally, this network integrates motor output across multiple cervical levels to produce stable yet adaptable control of head posture, vertebral alignment, and cervicothoracic transitions.
This reflects a shift from segmental innervation to coordinated biomechanical regulation.
Sensory Innervation
The cervical plexus provides cutaneous sensory innervation via its superficial branches (C2 – C4), forming an integrated afferent network supplying the neck, lower scalp, auricle, shoulder, and upper thoracic region.
These branches emerge at Erb’s point and represent redistributed segmental input organized into overlapping, non-dermatomal fields.
This arrangement ensures continuous sensory coverage and functional redundancy, allowing preservation of sensation despite partial root injury. Sensory modalities including touch, pain, and temperature are transmitted to the central nervous system, supporting protective reflexes and environmental awareness.
Functionally, this system transforms discrete spinal input into regionally integrated perception across the cervicothoracic interface.
Proprioception
Proprioceptive fibers from the cervical plexus convey afferent input from cervical muscles, joints, and associated connective tissues, forming a critical feedback system for position sense and movement coordination.
This input is essential for maintaining head orientation, balance, and dynamic postural control. Integration of proprioceptive feedback with motor output enables continuous adjustment of cervical muscle activity, ensuring precise alignment and smooth execution of movement.
This sensorimotor coupling supports higher-order functions such as gaze stabilization, coordinated respiration, and complex neck movements.
The multisegmental nature of these pathways enhances stability and resilience, allowing accurate neuromuscular control even under variable mechanical demands.
CLINICAL RELEVANCE
Phrenic Nerve Injury
Injury to the phrenic nerve (C3–C5), the principal motor output of the cervical plexus, results in diaphragmatic paralysis and loss of effective negative intrathoracic pressure generation. This directly compromises ventilation, reflecting the essential role of the plexus in respiratory control.
Unilateral lesions reduce ventilatory efficiency and may remain partially compensated by the contralateral diaphragm, whereas bilateral involvement leads to severe respiratory insufficiency requiring mechanical support.
The clinical impact highlights the dependence of life-sustaining respiration on intact cervical plexus function and its integration with thoracic biomechanics.
Cutaneous Disfunction
Involvement of the superficial sensory branches (C2–C4)- lesser occipital, great auricular, transverse cervical, and supraclavicular nerves – produces sensory disturbances across the neck, auricle, shoulder, and upper thoracic region.
Due to plexus-level redistribution, deficits are non-dermatomal and overlapping, typically presenting as diffuse hypoesthesia, paresthesia, or hypersensitivity rather than sharply localized loss.
Compression, trauma, or surgical irritation may disrupt afferent pathways, altering regional sensory mapping and impairing protective and proprioceptive feedback within the cervicothoracic interface.
Motor Disfunction
Damage to motor components of the cervical plexus, particularly the ansa cervicalis (C1–C3), impairs innervation of the infrahyoid muscles, disrupting hyoid stabilization and coordinated swallowing and phonation.
Additional involvement of prevertebral and scalene branches compromises cervical spine stability and coordinated neck movement.
Functionally, this reflects failure of integrated motor control, where segmentally derived fibers can no longer be effectively organized into coordinated biomechanical actions, leading to deficits in posture, airway maintenance, and cervicothoracic movement synchronization.
Cervical Relevance
Owing to its anatomical proximity to major cervical structures- including the carotid sheath (carotid artery, internal jugular vein) and deep cervical musculature – the cervical plexus holds significant clinical importance in surgical and interventional settings.
Cervical plexus blocks are widely used to provide regional anesthesia for procedures such as carotid endarterectomy and thyroid surgery, demonstrating its predictable anatomical organization.
However, this proximity also increases vulnerability to iatrogenic injury during surgical dissection or trauma, necessitating precise anatomical knowledge to preserve both motor and sensory function.