
Lumbar Plexus
The lumbar plexus is a fusion of the ventral rami of L1–L4 (± T12) of spinal nerves, organized within the posterior compartment of the psoas major muscle. It represents an early stage of peripheral nerve integration, where segmental spinal fibers undergo systematic division and recombination to create functionally coherent neural pathways.
Within the psoas major, each ramus splits into ascending and descending divisions, forming intersegmental connections that generate redundant, distributed motor and sensory output.
Branches emerge in a predictable topographic pattern:
Lateral border → anterior/lateral thigh – femoral innervation
Medial border → pelvic and medial thigh- obturator innervation
Anterior surface → – genitofemoral innervation
Functionally, the plexus supplies the anterior and medial lower limb compartments, mediating:
hip flexion ; knee extension; thigh adduction
Clinically, its intramuscular location within psoas major predisposes it to compression (e.g., hematoma, retroperitoneal pathology), producing plexus-level deficits- characteristically multisegmental, with combined motor and sensory impairment that does not conform to single root or terminal nerve distributions.
DESCRIPTION
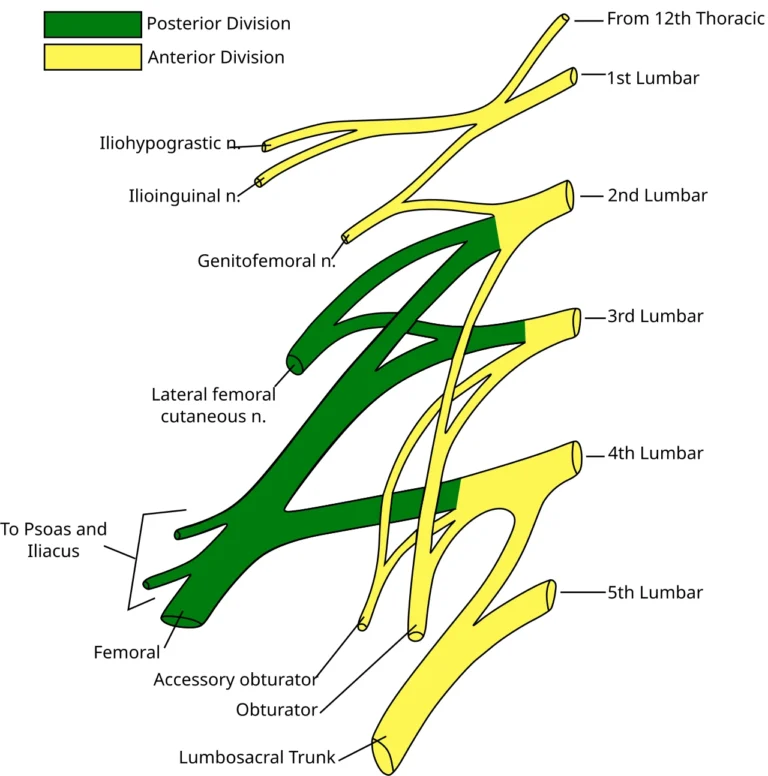
Lumbar Plexus Diagram” – Based on Gray822.svg (Gray’s Anatomy plate), modified by Mcstrother and Ninovolador, via Wikimedia Commons. Licensed under CC BY 3.0
AI-Generated Illustration-MyoAnatomy
Description
AI-Generated Illustration-MyoAntomy
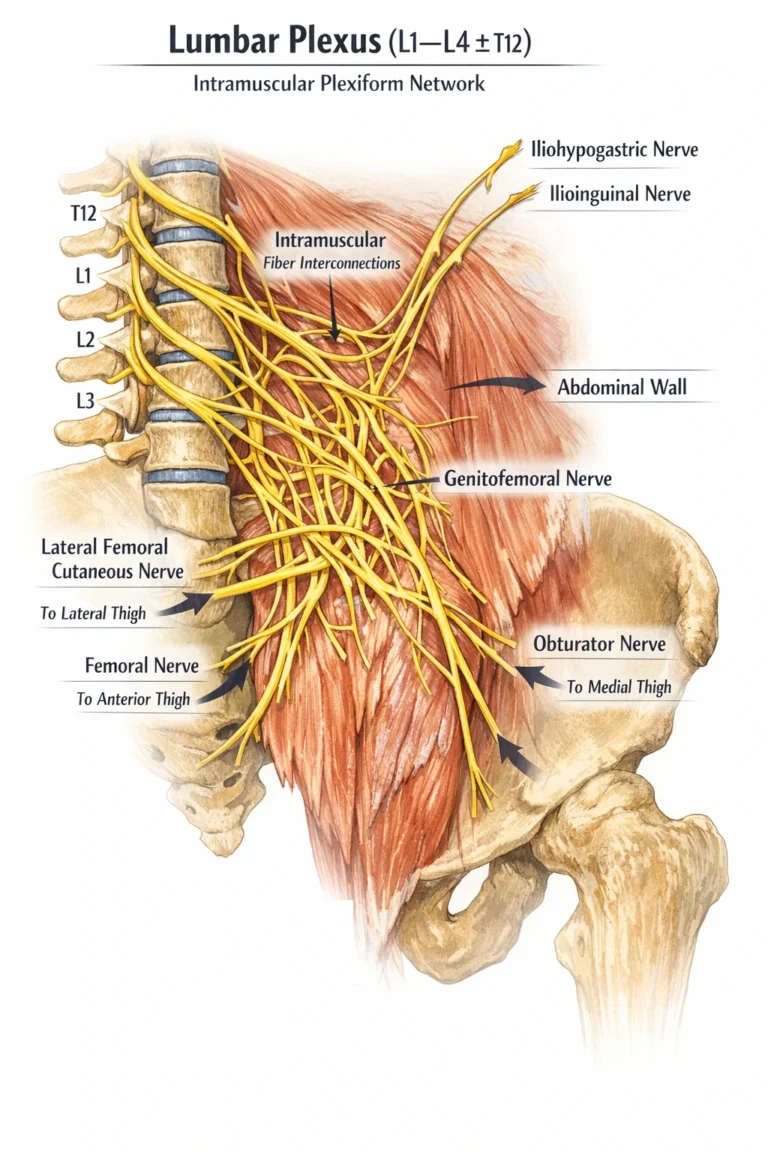
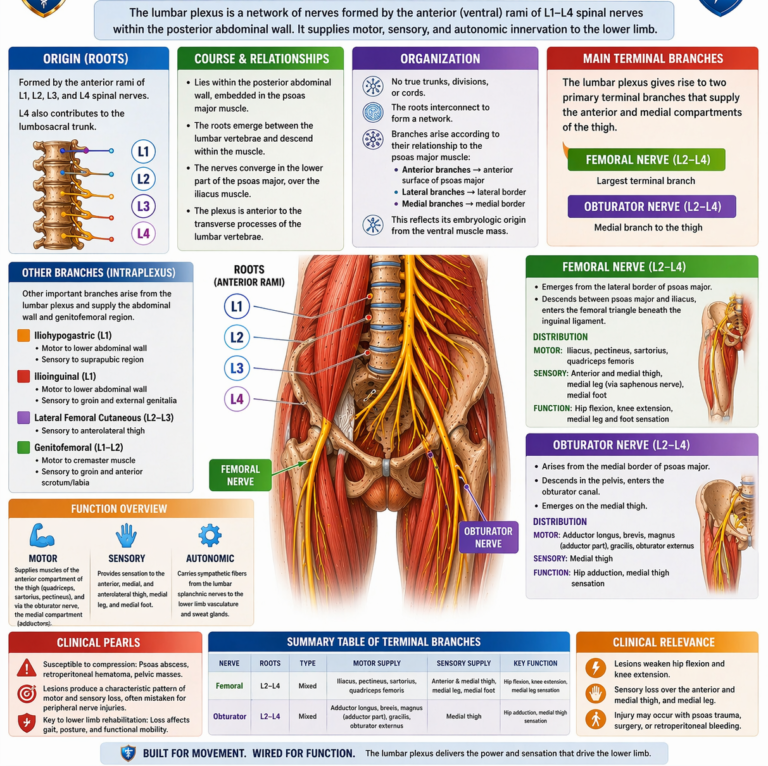
The lumbar plexus is a multisegmental intramuscular neural network formed by the fusion of the ventral rami of L1–L4 (± T12) of the spinal nerves within the posterior psoas major, representing an early plexiform stage of neural integration. In contrast to the hierarchical architecture of the brachial plexus, it lacks discrete trunks, divisions, and cords, instead demonstrating direct fiber convergence, recombination, and redistribution within muscle substance.
This organization reflects its derivation from the ventral embryological muscle mass, functionally biasing the plexus toward flexor and adductor systems of the anterior and medial compartments of the lower limb. Within psoas major, segmental fibers interconnect to form a dense functional syncytium, allowing early multisegmental integration prior to terminal nerve formation.
Branches emerge according to topographic and target-directed organization rather than sequential layering:
Superior (iliohypogastric, ilioinguinal) → abdominal wall
Anterior (genitofemoral nerve) → anterior thigh/genital region
Lateral (femoral, lateral femoral cutaneous nerves) → anterior/lateral thigh
Medial (obturator nerv) → medial thigh
Each terminal branch carries mixed GSE, GSA, and postganglionic sympathetic (GVE) fibers, integrating motor execution, somatosensory mapping, and autonomic vascular regulation.
Functionally, the plexus coordinates hip flexion, knee extension, and thigh adduction, forming the neural basis for closed-chain locomotion, postural stabilization, and trunk–pelvis–limb load transfer.
Inferiorly, L4 contributes to the lumbosacral trunk, linking the lumbar and sacral plexuses into a continuous functional axis for lower limb control.
Clinically, due to its intramuscular location, the plexus is vulnerable to compressive and retroperitoneal pathology. Lesions produce a plexopathy pattern – characterized by overlapping, non-dermatomal motor and sensory deficits, distinguishing it from radiculopathy (segmental/dermatomal) and mononeuropathy (peripheral nerve-specific).
Exam Question
Explain how the plexiform organization of the lumbar plexus, based on its embryological origin, enables early multisegmental integration, and relate this to patterns of motor control, fiber composition (GSE, GSA, GVE), and the clinical distinction between radiculopathy, plexopathy, and peripheral neuropathy.”
LATERAL BORDER
Description
AI-Generated Illustration-MyoAntomy
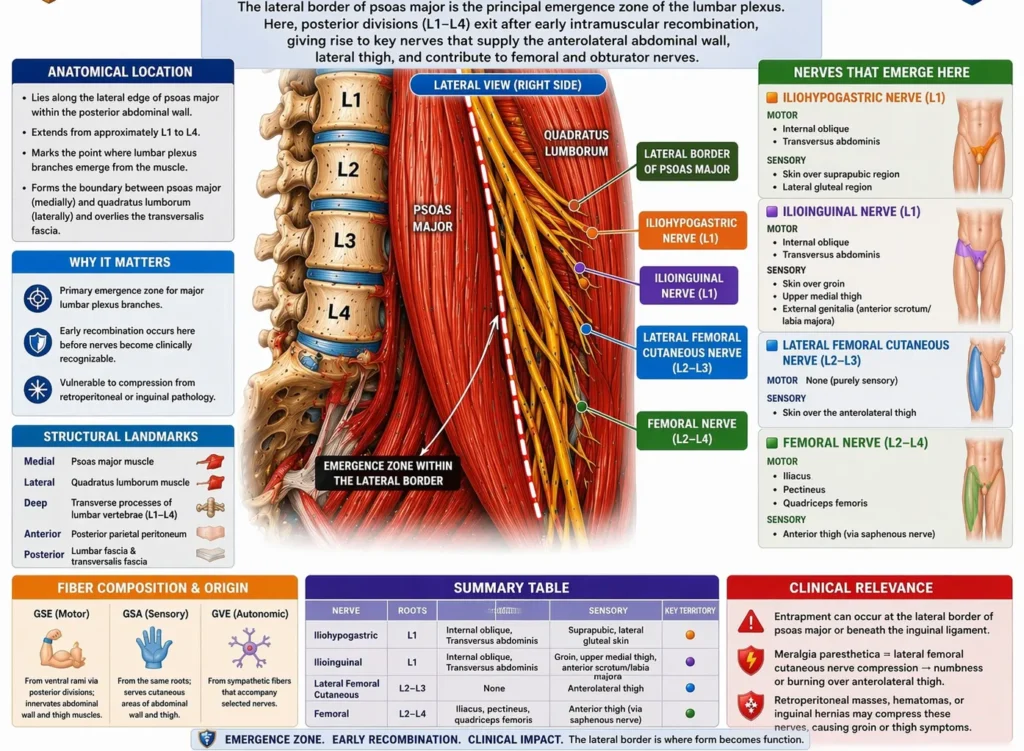
The lateral border of psoas major is a principal emergence zone of the lumbar plexus, where branches from the posterior divisions (L1–L4) exit after undergoing early intramuscular recombination within the plexiform network. Unlike hierarchical plexus organization, fibers here are already functionally sorted before emergence.
This region establishes the anterolateral abdominal wall and anterior thigh axis. Proximally, L1 branches (iliohypogastric, ilioinguinal) preserve segmental trunk innervation, while more caudal fibers (L2–L4) form integrated multijoint motor systems (notably via the femoral nerve), enabling coordinated hip flexion, knee extension, and postural stabilization essential for locomotion.
Fiber composition shows a functional gradient:
GSE (motor) → increases distally toward limb control
GSA (sensory) → maintains abdominal and thigh cutaneous mapping
GVE (sympathetic) → regulates vascular tone and sudomotor activity
Clinically, this border is a vulnerable topographic interface (psoas pathology, inguinal region compression). Lesions produce mixed multisegmental deficits, combining abdominal wall weakness, impaired hip flexion/knee extension, and sensory loss. This pattern distinguishes:
radiculopathy → segmental/dermatomal
plexopathy → multisegmental functional grouping
peripheral neuropathy → nerve-specific deficits
Exam Question
Analyze how lumbar plexus branches at the lateral border of psoas major reflect early fiber recombination and enable the transition from segmental trunk innervation to integrated lower limb control, including implications for fiber composition and differentiation of radiculopathy, plexopathy, and peripheral nerve lesions.”
Iliohypogastric
The iliohypogastric nerve is a mixed peripheral nerve of the lumbar plexus arising from L1, containing:
GSE (general somatic efferent) – motor to anterolateral abdominal wall musculature
GSA (general somatic afferent) – sensory from suprapubic and gluteal regions
GVE (postganglionic sympathetic) – autonomic fibers to cutaneous structures
It emerges from the lateral border of psoas major, crosses quadratus lumborum, pierces transversus abdominis, and continues between abdominal wall layers before dividing into terminal cutaneous branches.
At a systems level, the nerve represents an early segmental output of the lumbar plexus, transmitting predominantly L1-derived ventral motor pool activity to the abdominal wall.
Functionally, it contributes to:
Abdominal wall contraction (internal oblique, transversus abdominis)
Intra-abdominal pressure generation
Core stabilization and trunk support
Its sensory component supplies the suprapubic region and posterolateral gluteal skin, linking motor stabilization with localized somatosensory mapping.
Clinically, injury results in weakness of abdominal wall tone and impaired pressure regulation, with sensory loss in its cutaneous territory. Deficits remain segmental, reflecting its limited integration within the plexus.
Exam Question
Explain how the iliohypogastric nerve reflects segmental organization of the lumbar plexus, and analyze how its fiber composition (GSE, GSA, GVE) supports abdominal wall biomechanics, intra-abdominal pressure regulation, and proximal trunk stabilization.”
Illiioinguinal
The ilioinguinal nerve is a mixed peripheral nerve of the lumbar plexus arising from L1, containing:
GSE (general somatic efferent) – motor to lower abdominal wall (minor contribution)
GSA (general somatic afferent) – sensory from inguinal region and external genitalia
GVE (postganglionic sympathetic) – autonomic fibers to cutaneous structures
It emerges inferior to the iliohypogastric nerve, follows a similar course across the posterior abdominal wall, and enters the inguinal canal, exiting via the superficial inguinal ring.
At a systems level, it represents a regionally specialized extension of L1 segmental output, with greater emphasis on somatosensory distribution rather than motor dominance.
Functionally, it contributes to:
Lower abdominal wall support (internal oblique, transversus abdominis)
Somatosensory mapping of the inguinal and genital regions
Integration of trunk stabilization with peripheral sensory feedback
Its sensory territory includes the upper medial thigh and external genitalia, forming part of the inguinal sensory network.
Clinically, it is vulnerable during inguinal surgical procedures, where injury leads to groin pain, paresthesia, or sensory loss, often presenting as postoperative neuralgia. Functional deficits are subtle due to overlap with adjacent nerves.
Exam Question
Analyze how the ilioinguinal nerve represents a regionally specialized extension of L1 output, and discuss how its fiber composition and anatomical course enable integration of lower abdominal wall function with somatosensory mapping of the inguinal and external genital regions.”
Lateral Femoral Cutaneous Nerve
The lateral femoral cutaneous nerve is a pure somatic afferent (GSA) branch of the lumbar plexus, arising from the posterior divisions of L2–L3 and emerging from the lateral border of psoas major. It courses obliquely across the iliacus, passes beneath or through the inguinal ligament near the ASIS, and enters the thigh as a purely cutaneous nerve.
Functionally, it represents a selectively routed sensory pathway, carrying modality-specific input (touch, pain, temperature) from the anterolateral thigh, without participation in motor control.
Topographically, its superficial course at the inguinal ligament makes it uniquely vulnerable to mechanical compression, particularly at the osteofibrous tunnel near the ASIS. Because it lacks motor fibers, lesions produce pure sensory deficits without weakness, preserving motor function of the limb.
Clinically, this underlies meralgia paresthetica, characterized by burning pain, paresthesia, or numbness over the lateral thigh, often exacerbated by increased intra-abdominal pressure or external compression (tight clothing, obesity, pregnancy). The condition exemplifies isolated peripheral sensory neuropathy within an otherwise intact motor system.
Exam Question
Analyze how the lateral femoral cutaneous nerve demonstrates selective GSA fiber routing within the lumbar plexus, and explain how its anatomical course predisposes it to entrapment, correlating this with the pathophysiology and purely sensory clinical presentation of meralgia paresthetica.”
Femoral Nerve
The femoral nerve is the largest terminal branch of the lumbar plexus, formed from the posterior divisions of L2–L4, carrying mixed fibers (GSE + GSA). It emerges from the lateral border of psoas major, descends between psoas major and iliacus, and passes deep to the inguinal ligament into the femoral triangle, where it divides into multiple motor and sensory branches.
Functionally, it represents a major multisegmental motor output pathway, integrating fibers that have undergone early recombination within the lumbar plexus. Its motor (GSE) fibers innervate the anterior compartment of the thigh (quadriceps femoris, sartorius, iliacus, and partially pectineus), forming the principal axis for knee extension and hip flexion, essential for locomotion, posture, and load transfer.
Its sensory (GSA) component provides cutaneous innervation to the anterior thigh and, via the saphenous nerve, to the medial leg and foot, establishing a continuous somatosensory map aligned with its motor domain. This integration reflects coordinated distribution of motor and sensory fibers within a single functional system.
Clinically, femoral nerve lesions produce weakness of knee extension, diminished hip flexion, and loss of the patellar reflex (L3–L4), accompanied by sensory deficits in its cutaneous territory.
Exam Question
“Explain how the femoral nerve integrates multisegmental GSE and GSA fibers to coordinate anterior thigh motor function and somatosensory mapping, and analyze how this organization determines the biomechanical and clinical consequences of lesions at root, plexus, and peripheral nerve levels’.”
MEDIAL BORDER
Description
AI-Generated Illustration-MyoAntomy
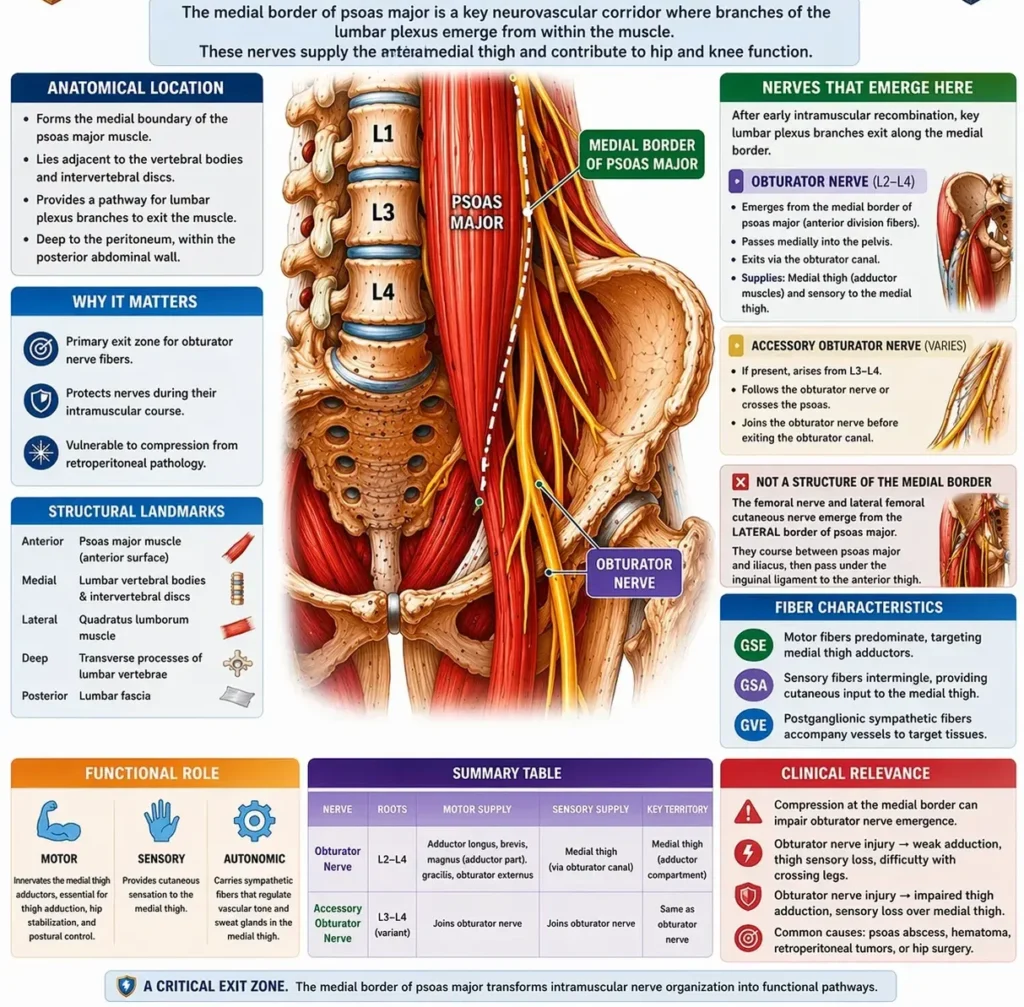
The medial border of psoas major gives rise to neural elements derived predominantly from the anterior divisions of L1–L4, reflecting their embryological association with hypaxial musculature of the medial compartment.
These fibers reorganize early within the intramuscular plexiform network and emerge as functionally targeted pathways directed toward the pelvis and medial thigh, most prominently via the obturator and genitofemoral nerves.
Its fiber composition includes integrated GSE (motor), GSA (sensory), and GVE (postganglionic sympathetic) components.
GSE fibers form coordinated motor pools supplying medial thigh adductors, mediating thigh adduction and coronal plane stabilization, particularly during the stance phase of gait.
GSA fibers provide cutaneous innervation of the medial thigh and articular input from the hip and knee, contributing to proprioceptive feedback essential for midline alignment and load transfer. GVE fibers regulate regional vascular tone, linking autonomic modulation to somatic function.
At a systems level, the medial border represents a medial stabilizing axis, where multisegmental lumbar output is integrated into a pathway specialized for control of medial limb positioning, prevention of lateral pelvic drift, and dynamic stabilization during locomotion. This contrasts with lateral outputs that prioritize flexor–extensor propulsion, emphasizing instead fine coronal plane control and postural equilibrium.
Topographically, these nerves descend along the lateral pelvic wall and traverse confined spaces such as the obturator canal, creating anatomically restricted corridors prone to compression. Because fibers are already selectively organized, lesions produce compartment-specific deficits, most notably adductor weakness and medial sensory loss.
Clinically, pathology at this level produces patterns consistent with plexus-derived peripheral neuropathy, distinguishable from radiculopathy by loss of segmental patterning and from distal nerve lesions by preservation of non-medial compartments. This reflects disruption of an integrated multisegmental pathway localized to the medial lumbar plexus output.
Exam Question
“Analyze how the medial border of the lumbar plexus reflects embryologically determined anterior-division fiber organization, and explain how its GSE, GSA, and GVE components integrate to control medial thigh function, coronal plane stability, and the characteristic clinical distinction between radiculopathy, plexopathy, and peripheral nerve lesions.”
Obturator Nerve
The obturator nerve is a mixed peripheral nerve of the lumbar plexus arising from the anterior divisions of L2–L4, carrying integrated GSE (motor), GSA (sensory), and GVE (sympathetic) fibers.
It emerges from the medial border of psoas major, descends along the lateral pelvic wall, and traverses the obturator canal to enter the medial compartment of the thigh, where it typically divides into anterior and posterior branches separated by adductor brevis, reflecting organized intramuscular fiber redistribution.
At a systems level, the nerve represents a selectively integrated medial motor–sensory pathway, in which multisegmental lumbar fibers are functionally sorted to supply the adductor muscle group. Its GSE fibers form a coordinated motor pool responsible for thigh adduction, assisted hip flexion, and fine coronal plane stabilization, while its GSA fibers provide cutaneous input from the medial thigh and articular feedback from the hip and knee joints, contributing to proprioceptive regulation of lower limb alignment.
Functionally, the obturator nerve defines the medial stabilizing axis of the lower limb, coordinating adductor activity to control midline positioning and load transfer during gait, particularly in single-limb stance and directional movement. The inclusion of GVE fibers supports regional vascular tone, integrating autonomic modulation with somatic function.
Topographically, its deep pelvic course and passage through the obturator canal create a confined anatomical corridor, making it susceptible to compression or injury in pelvic pathology. Because its fibers are organized into a discrete medial compartment output.
Clinically, obturator nerve injury results in impaired thigh adduction, reduced coronal plane stability, and sensory loss over the medial thigh. Causes include pelvic surgery, obturator canal entrapment, and obturator hernia, illustrating a localized plexus-derived neuropathy.
Exam Question
“Analyze how the obturator nerve integrates L2–L4 fibers into a medial compartment motor–sensory pathway, and explain how its fiber composition and anatomical course determine its role in coronal plane stabilization and the clinical pattern of obturator nerve lesions.”
ANTERIOR SURFACE
Description
AI-Generated Illustration-MyoAntomy
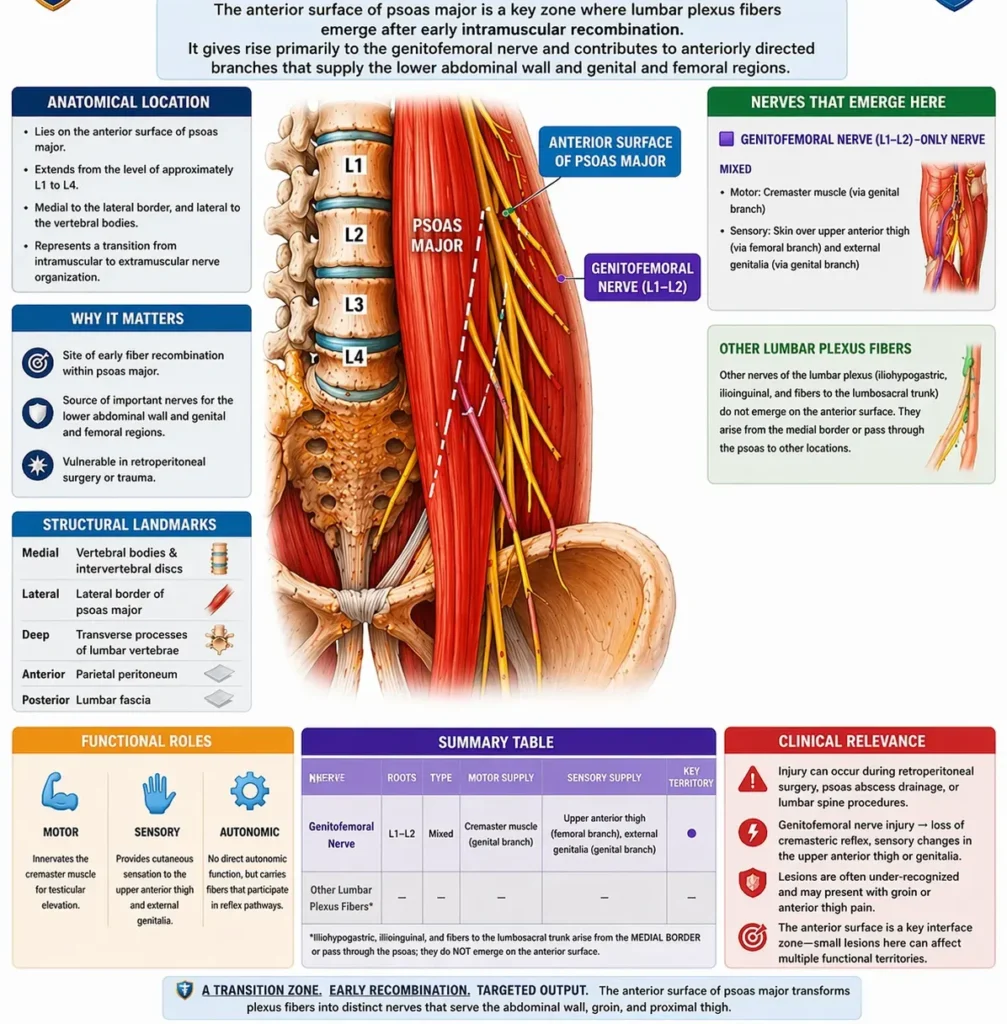
The anterior surface of the lumbar plexus is characterized by the emergence of selectively routed neural pathways onto the anterior aspect of psoas major, representing a transition from intramuscular plexiform organization to target-directed peripheral distribution.
The genitofemoral nerve (L1–L2) is the principal structure of this surface, arising from the anterior divisions and appearing directly on the anterior surface of psoas major, where it descends vertically before dividing into genital and femoral branches. This unique emergence reflects early segregation of fibers destined for inguinal, genital, and proximal anterior thigh territories.
Functionally, the anterior surface represents a viscerosomatic interface zone, integrating:
GSA fibers → cutaneous sensation from inguinal and proximal femoral regions
GSE fibers → focal motor output (cremaster muscle)
GVE fibers → autonomic regulation of regional vasculature
This organization enables rapid reflex integration, most notably the cremasteric reflex (L1–L2), linking sensory input from the thigh with motor output to the cremaster, demonstrating tight coupling between somatic sensation and reflex motor control.
Topographically, the superficial position of these fibers on psoas major predisposes them to mechanical and iatrogenic injury, particularly in retroperitoneal procedures, with lesions producing localized sensory deficits and reflex impairment rather than major motor dysfunction.
At a systems level, the anterior surface differs from lateral and medial borders by emphasizing sensory-reflex specialization and visceral interface function, rather than large-scale locomotor control
Exam Question
Explain how the anterior surface of the lumbar plexus reflects selective fiber routing for viscerosomatic integration, and analyze how this organization underlies the cremasteric reflex and the clinical pattern of anterior plexus lesions.”
Genitofemoral Nerve
The genitofemoral nerve is a mixed peripheral nerve arising from the anterior divisions of L1–L2, containing integrated GSE (motor), GSA (sensory), and GVE (postganglionic sympathetic) fibers.
It emerges uniquely on the anterior surface of psoas major, reflecting early intramuscular fiber recombination and a direct anterior projection of lumbar plexus output. It descends vertically and divides into genital and femoral branches, representing functionally distinct but developmentally linked pathways.
At a systems level, the nerve functions as an interface between somatic and viscerosomatic domains, integrating lower abdominal wall, inguinal, and external genital innervation.
Its GSE fibers are limited and primarily directed to the cremaster muscle, forming the efferent limb of the cremasteric reflex.
GSA fibers provide cutaneous innervation to the anterior scrotum (♂) or labia majora (♀) via the genital branch and to the upper anterior thigh via the femoral branch.
GVE fibers contribute to autonomic regulation of regional vasculature, linking sensory and reflexive responses.
Functionally, the genitofemoral nerve mediates protective reflex integration, most notably the cremasteric reflex (L1–L2), coupling sensory input from the proximal thigh to motor contraction of the cremaster, thereby participating in thermoregulatory and protective testicular responses. It also contributes to somatosensory mapping of the inguinal region, bridging abdominal wall and proximal limb innervation.
Topographically, its course on the anterior surface of psoas major makes it particularly vulnerable to retroperitoneal compression or surgical injury, and its division near the inguinal region creates anatomically distinct territories that can be selectively affected.
Clinically, lesions produce loss of the cremasteric reflex, sensory deficits in the genital region and upper anterior thigh, and may present with inguinal pain syndromes. Because of its mixed but limited motor function, deficits are predominantly sensory-reflex in nature, reflecting disruption of a specialized viscerosomatic integration pathway.
Exam Question
Analyze how the genitofemoral nerve integrates L1–L2 anterior-division fibers into a viscerosomatic pathway, and explain how its GSE, GSA, and GVE components underlie the cremasteric reflex, regional sensory distribution, and the clinical pattern of genitofemoral nerve lesions.”
FUNCTIONAL IMPORTANCE
Motor Control
The lumbar plexus constitutes the principal multisegmental ventral motor outflow to the lower limb, especially through L2–L4, organizing neural drive to muscle groups responsible for hip flexion, thigh adduction, and knee extension.
Its largest motor contribution is through the femoral nerve, which supplies the anterior thigh and establishes the dominant sagittal-plane locomotor axis. Iliopsoas-mediated hip flexion initiates limb advancement during swing, while quadriceps-mediated knee extension stabilizes the limb during stance and weight acceptance.
Medial plexus outputs, particularly via the obturator nerve, supplement this system by controlling coronal plane alignment and preventing excessive pelvic drift.
Functional impact: provides the neural basis for propulsion, load acceptance, and lower-limb postural stabilization during locomotion.
Sensory Mapping
The lumbar plexus carries integrated GSA afferent pathways from the lower abdominal wall, inguinal region, anterior thigh, medial thigh, and parts of the medial leg, creating a regionally organized sensory map through the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, obturator, and femoral nerves.
These fibers transmit modality-specific input, including touch, pressure, pain, temperature, and deep articular sensation, allowing the CNS to continuously monitor surface contact, tissue injury, and joint-related sensory information.
Although individual cutaneous territories vary, the plexus as a whole establishes a functional sensory field aligned with the biomechanics of the trunk–pelvis–thigh unit.
Functional impact: supports protective sensation, spatial orientation, and sensorimotor coupling required for safe and adaptive lower-limb use.
Proprioceptive Integration
The lumbar plexus conveys deep afferent information from muscle spindles, Golgi tendon organs, joint capsules, and periarticular mechanoreceptors, particularly from the hip and knee regions. This proprioceptive inflow provides real-time data regarding joint angle, muscle length, tension, and mechanical loading, allowing continuous refinement of motor output.
Through this feedback loop, lumbar plexus pathways help synchronize agonist-antagonist activity, regulate limb stiffness, and adapt motor patterns to changing terrain or load.
This is particularly important during the transition from stance to swing, when precision of limb position must be maintained despite dynamic shifts in body mass.
Functional impact: enables fine movement calibration, postural correction, and mechanical efficiency through closed-loop neuromuscular control.
Gait Dynamics
The lumbar plexus integrates motor and sensory elements into a coordinated network essential for upright bipedal gait. Motor output drives the major proximal actions of locomotion, while sensory and proprioceptive input continuously modulate timing, force generation, and limb positioning.
During gait, the plexus contributes to pelvic stabilization, controlled hip flexion, knee stabilization in stance, and efficient limb advancement in swing. Its pathways therefore do not act as isolated nerves, but as components of a broader biomechanical system that couples trunk stability, center-of-gravity control, and lower-limb progression.
Because the lumbar plexus is especially important proximally, its integrity is critical for maintaining the transition between weight-bearing stability and forward movement.
Functional impact: enables stable, adaptive, and energy-efficient locomotion across varying mechanical demands.
CLINICAL RELEVANCE
Lumbar Plexopathy
Lumbar plexopathy reflects pathology within the posterior abdominal wall/retroperitoneal space, disrupting multisegmental ventral rami (L1–L4 ± T12) after intraplexus recombination. Because fibers are already integrated, lesions produce combined motor–sensory deficits across multiple terminal distributions, rather than isolated nerve patterns.
Motor impairment involves the coordinated loss of hip flexion (iliopsoas, L1–L2), knee extension (quadriceps, L2–L4), and thigh adduction (obturator system, L2–L4), while sensory deficits span overlapping anterior and medial thigh territories. Reflex involvement, particularly patellar reflex attenuation (L3–L4), reflects disruption of integrated segmental loops.
Clinical significance: represents failure of a distributed neuromuscular network, producing non-dermatomal, multinerve deficits, distinguishing plexopathy from radiculopathy (segmental) and peripheral neuropathy (focal).
Motor Nerve Injury
Injury to individual lumbar plexus branches produces selective disruption of functionally organized motor pools, reflecting prior fiber sorting within the plexus.
Femoral nerve (L2–L4): loss of quadriceps function → impaired knee extension, reduced stance-phase stability, diminished weight acceptance, and decreased patellar reflex
Obturator nerve (L2–L4): weakness of thigh adduction, compromising coronal plane stabilization and pelvic control
These deficits disrupt coordinated activation across proximal joints, particularly during load transfer and stance stabilization.
Clinical significance: demonstrates how injury to a single terminal nerve selectively impairs a specific biomechanical axis (sagittal vs coronal), while preserving other plexus functions.
Sensory Neuropathy
Selective involvement of pure GSA pathways within the lumbar plexus produces isolated sensory neuropathies, exemplified by compression of the lateral femoral cutaneous nerve (L2–L3) at the inguinal ligament. This results in meralgia paresthetica, characterized by dysesthesia over the anterolateral thigh without motor involvement.
This pattern reflects the functional independence of terminal sensory branches, despite proximal fiber integration, and highlights vulnerability at anatomical transition zones, where nerves become superficial and mechanically exposed.
Clinical significance: defines a pure afferent lesion, preserving motor output and enabling clear distinction from plexus or root pathology.
Surgical Risk
The lumbar plexus lies within psoas major and adjacent retroperitoneal planes, making it susceptible during pelvic, spinal, retroperitoneal, and hip procedures, as well as regional anesthesia. Because lesions occur after multisegmental integration, deficits are diffuse, overlapping, and non-dermatomal, often involving both motor and sensory systems.
Patterns include combined impairment of hip flexion, knee extension, and thigh adduction, alongside broad sensory disturbances and reflex changes. These reflect disruption of integrated motor pools and distributed sensory mapping, rather than isolated pathways.
Clinical significance: accurate localization depends on recognizing plexus-level injury patterns, where deficits are multisegmental and functionally integrated, in contrast to root or single-nerve lesions.