
Brachial Plexus
The brachial plexus is a multisegmental redistribution network formed by the anterior (ventral) rami of C5–Th1 spinal nerves, in which spinal fibers are reorganized into functionally specialized peripheral pathways for the upper limb. Through its hierarchical structure – roots, trunks, divisions, cords, and terminal branches – the plexus converts segmental spinal input into integrated motor, sensory, and sympathetic output.
Its essential function is to provide coordinated innervation of the shoulder girdle and upper limb, allowing proximal stability, distal dexterity, and continuous sensorimotor feedback. Because fibers from several spinal levels contribute to individual peripheral nerves, the plexus creates multisegmented innervation and partial functional redundancy, which improves precision of movement but also produces characteristic non-simple patterns of deficit in plexus injury.
Anatomically, it extends from the lower cervical region to the axilla, passing between the anterior and middle scalene muscles, behind the clavicle, and around the axillary artery, whose relation is especially important at the cord level.
Clinically, the brachial plexus is best understood as an interface between segmental spinal organization and regional limb function: proximal lesions disturb broad biomechanical patterns, whereas distal lesions increasingly affect target-specific motor and sensory teritories.
BRANCHES
Brachial Plexus (Anterior View)” – Modified by Mattopeedia, derived from Gray’s Anatomy (1918), further edits by Captain-n00dle & MissMJ, Wikimedia Commons. Public Domain
AI-Generated Illustration-MyoAnatomy
Description
AI-Generated Illustration-MyoAnatomy
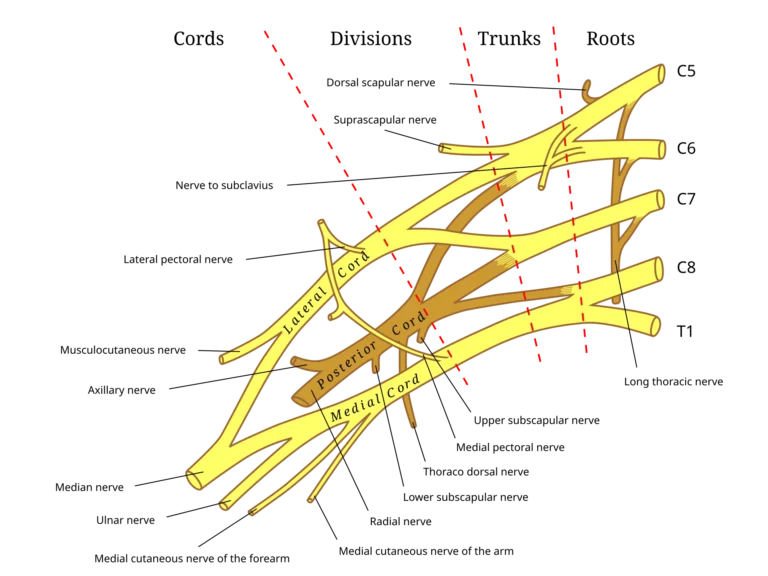
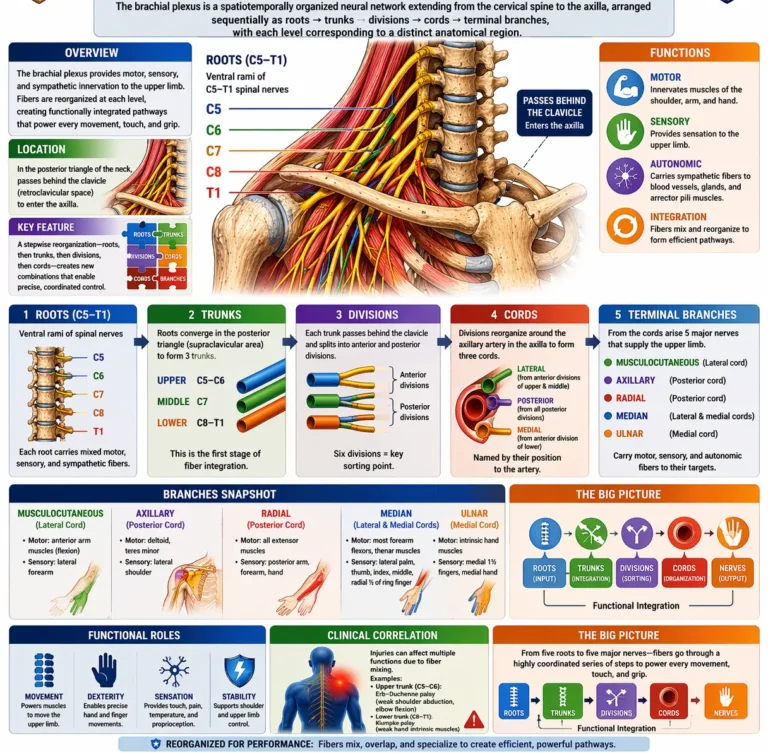
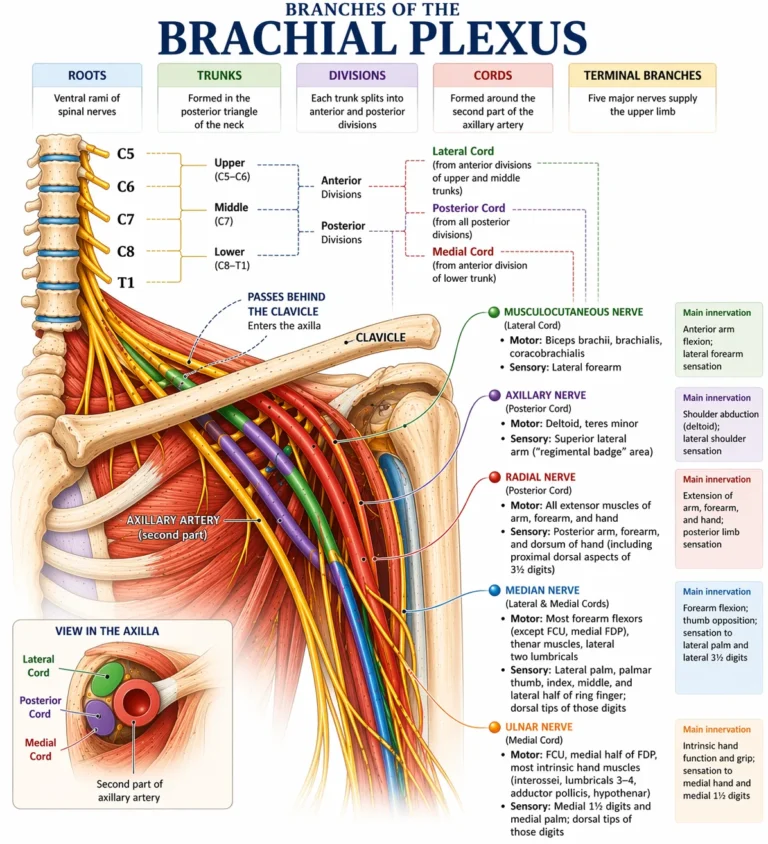
The brachial plexus is a spatiotemporally organized neural network extending from the cervical spine to the axilla, arranged sequentially as roots → trunks → divisions → cords → terminal branches, with each level corresponding to a distinct anatomical region. In the interscalene triangle of the neck, the ventral rami (C5–T1) form the roots, which converge in the supraclavicular region to form trunks, representing the first stage of fiber integration.
As the plexus passes through the retroclavicular region, each trunk divides into anterior and posterior divisions, establishing functional segregation aligned with flexor and extensor compartments. Distally, within the axilla, these divisions reorganize around the second part of the axillary artery to form cords, reflecting a key topographic transition where fibers are selectively recombined into functionally coherent bundles. Beyond this, terminal branches extend into the upper limb, carrying a multisegmental distribution of fibers that enables coordinated multijoint motor control and integrated somatosensory mapping.
Exam Question
Explain how the sequential organization of the brachial plexus (roots → trunks → divisions → cords → terminal branches) reflects a transition from segmental spinal output to functionally integrated neural pathways, and analyze how the processes of fiber segregation at the division level and recombination at the cord level enable coordinated multijoint motor control and integrated somatosensory distribution in the upper limb.
Roots
The roots of the brachial plexus are formed by the anterior (ventral) rami of C5–Th1, emerging from the intervertebral foramina and passing laterally through the interscalene interval between the anterior and middle scalene muscles, superior to the first rib.
At this level, fibers retain strict segmental identity, representing the direct, unrecombined continuation of spinal cord output.
Each root carries mixed fibers:
GSE (somatic motor) from ventral horn motor neurons
GSA (somatic sensory) from dorsal root ganglia
GVE (postganglionic sympathetic)
Functionally, the roots constitute the primary segmental input layer, transmitting signals that preserve the organization of ventral horn motor pools, which are arranged longitudinally and somatotopically (proximal–distal, flexor–extensor). Because no plexus-level redistribution has yet occurred, myotomal and dermatomal patterns remain intact, with minimal redundancy.
Consequently, root lesions produce precise segmental deficits, characterized by localized motor weakness and dermatomal sensory loss. This reflects the absence of fiber recombination and direct mapping to spinal segment function.
Despite this, early functional specialization is already evident through collateral branches:
Dorsal scapular nerve (C5) → rhomboids, levator scapulae (scapular retraction/elevation)
Long thoracic nerve (C5–C7) → serratus anterior (scapular stabilization and upward rotation)
These branches indicate prioritization of proximal postural and stabilizing control before plexus integration.
Anatomically, roots are vulnerable to radiculopathy, traction, and scalene compression, producing deficits that directly reflect their segmental organization. Injury to the long thoracic nerve results in scapular winging, emphasizing the clinical relevance of early branching.
In summary, the roots represent the pure segmental stage of the plexus, preserving spinal motor and sensory architecture while initiating selective output to key stabilizing muscles, forming the foundation for subsequent integration at higher plexus levels.
Exam Question
Explain why root-level lesions produce highly segmental deficits, relating this to preservation of motor pool organization, absence of fiber recombination, and the functional significance of early collateral branches.level lesions.
Trunks
The trunks of the brachial plexus are formed in the posterior triangle of the neck, superior to the clavicle, by convergence of the anterior rami of C5–Th1 into three units: the upper trunk (C5–C6), middle trunk (C7), and lower trunk (C8–Th1). This stage represents the first structured recombination of spinal fibers, marking the transition from strictly segmental output to integrated limb-oriented organization.
At this level, fibers from adjacent spinal segments merge into shared motor pools derived from ventral horn neuron columns. This recombination preserves functional identity (proximal–distal, flexor–extensor bias) while redistributing it across multiple segments, enabling coordinated multi-joint activation and introducing functional redundancy. Consequently, segmental precision is reduced compared to the root level, but integrated motor control is enhanced.
A proximal–distal functional gradient is established. The upper trunk (C5–C6) is biased toward proximal musculature, particularly shoulder stabilization and initiation of movement. The middle trunk (C7) functions as a central integrative conduit linking proximal and distal systems. The lower trunk (C8–Th1) is biased toward distal musculature, especially intrinsic hand function requiring fine motor precision. This reflects the intrinsic somatotopic organization of motor neuron pools within the spinal cord.
Branches arising from the trunk level demonstrate early specialization.
The suprascapular nerve (C5–C6) supplies supraspinatus and infraspinatus, enabling initiation of abduction and external rotation, while the
Nerve to subclavius (C5–C6) stabilizes the clavicle, supporting force transmission across the shoulder girdle. These branches indicate that proximal stabilization and movement initiation are established prior to further redistribution.
Clinically, trunk lesions produce deficits that are broader than root-level injuries due to partial recombination, yet not confined to individual peripheral nerve territories. For example, an upper trunk lesion disrupts C5–C6-derived motor pools, leading to weakness of shoulder abduction, external rotation, and elbow flexion, classically presenting as the “waiter’s tip” posture. This reflects loss of integrated multi-segmental function rather than isolated segmental or terminal nerve deficits.
In summary, the trunks represent the first integrative layer of the plexus, where segmental spinal output is reorganized into coordinated, multi-segmental functional units, establishing redundancy and preparing for functional sorting at the division level.
Exam Question
Explain how the trunk level of the brachial plexus represents the transition from segmental to integrated motor control, and discuss how recombination of adjacent spinal fibers influences motor pool organization, functional redundancy, and the clinical pattern of trunk-level lesions.
Devisions
The divisions of the brachial plexus are formed posterior to the clavicle as each trunk bifurcates into anterior and posterior divisions, producing six divisions in total. This stage represents the primary functional sorting layer, where previously integrated multi-segmental fibers are reorganized according to their ultimate participation in limb compartment function.
At this level, neural organization shifts from regional integration to functional compartmentalization. Anterior divisions transmit fibers destined for flexor-pronator systems of the anterior compartments, while posterior divisions transmit fibers to extensor-supinator systems of the posterior compartments. This separation reflects preservation of embryologically distinct ventral and dorsal motor pools, originating from ventral horn neuron columns and maintained despite earlier recombination.
The division level encodes the consequences of embryological limb rotation, in which the upper limb undergoes lateral rotation, repositioning ventral musculature anteriorly and dorsal musculature posteriorly. Thus, divisions act as a functional sorting interface, ensuring that motor and sensory fibers are directed into coherent biomechanical systems rather than maintaining segmental grouping.
Clinically, lesions at the division level produce compartment-based deficits, affecting either flexor or extensor systems across multiple joints. Because segmental identity has already been lost and terminal nerve organization has not yet formed, deficits appear functionally distributed rather than dermatomal or nerve-specific.
Exam Question
Explain how the division level of the brachial plexus serves as a functional sorting interface, and discuss how embryological limb rotation and preservation of ventral versus dorsal motor pools determine the organization of flexor and extensor systems, including the clinical implications of division-level lesions.
Cords
The cords of the brachial plexus are formed in the axilla by recombination of the divisions around the axillary artery and are named according to their positional relationship to this vessel: lateral, medial, and posterior cords.
The lateral cord is formed from anterior divisions of the upper and middle trunks (C5–C7), the medial cord from the anterior division of the lower trunk (C8–Th1), and the posterior cord from all three posterior divisions (C5–T1). At this level, fibers from multiple spinal segments and functional groups are combined into neurovascularly aligned bundles.
Functionally, the cords consolidate fibers into multi-segmental motor and sensory pools that will be distributed through terminal nerves, ensuring both functional redundancy and coordinated activation across compartments and joints. This organization enables each terminal nerve to carry contributions from multiple spinal levels.
Collateral branches arising from the cords reflect progressive specialization of proximal control. The lateral and medial pectoral nerves coordinate pectoral musculature, medial cutaneous nerves supply the arm and forearm, and branches of the posterior cord (subscapular and thoracodorsal nerves) supply major stabilizing and power-generating muscles of the posterior shoulder and back. These branches demonstrate that proximal control is refined before distal distribution via terminal nerves.
Clinically, cord lesions produce complex, multi-nerve deficits, as fibers from multiple roots and functional systems have already been integrated. For example, posterior cord injury leads to widespread extensor dysfunction, including loss of shoulder abduction (axillary nerve) and forearm/wrist extension (radial nerve), illustrating the integrated nature of this level.
Exam Question
Explain how the cord level of the brachial plexus integrates functionally sorted fibers into terminal nerve distributions, and discuss how their anatomical relationship to the axillary artery reflects their role in coordinating multi-segmental motor pools, including the clinical consequences of cord-level lesions.
LATERAL CORD
Description
AI-Generated Illustration-MyoAntomy
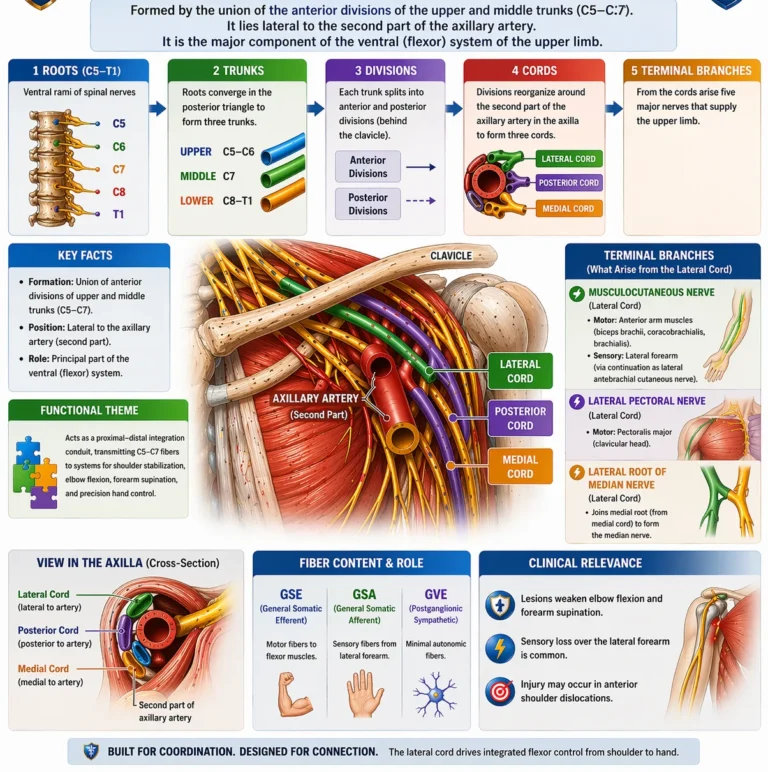
The lateral cord of the brachial plexus is formed by the union of the anterior divisions of the upper and middle trunks (C5–C7) and is positioned lateral to the second part of the axillary artery. It represents a principal component of the ventral (flexor) system, containing s a mixed population of neural fibers, including
GSE (general somatic efferent) motor fibers from ventral horn neurons,
GSA (general somatic afferent) sensory fibers from peripheral receptors,
GVE (postganglionic sympathetic) autonomic fibers.
Functionally, it is dominated by GSE fibers supplying the ventral (flexor) system of the upper limb, particularly the anterior arm, while its sensory and autonomic components are conveyed distally through its terminal branches (musculocutaneous and median nerves).
At this stage, fibers derived from ventral horn motor pools have undergone both segmental recombination (trunks) and functional compartmentalization (divisions). The lateral cord therefore carries multi-segmental, functionally coherent motor pools destined for flexor-pronator systems. This organization enables coordinated activation across proximal and distal joints.
Functionally, the lateral cord acts as a proximal–distal flexor integration conduit, transmitting C5–C7 fibers into systems responsible for shoulder stabilization, elbow flexion, and forearm supination, while also contributing to precision hand control via the median nerve. This reflects a hierarchical motor strategy in which proximal positioning of the limb is integrated with distal manipulation, ensuring efficient execution of goal-directed movements.
Its principal branches—the lateral pectoral nerve, musculocutaneous nerve, and lateral root of the median nerve – demonstrate progressive distribution of this integrated output. The lateral pectoral nervesupports anterior shoulder girdle stabilization and force transmission, the musculocutaneous nerve supplies the primary flexion-supination apparatus of the arm, and the lateral root of the median nerve conveys upper-segment fibers into the median nerve, extending this ventral system into the forearm and hand.
Clinically, lesions of the lateral cord disrupt a coherent flexor functional network rather than a single segment or peripheral nerve. This results in weak elbow flexion and supination, impaired shoulder flexion/adduction, and partial median nerve dysfunction, particularly affecting proximal median-innervated muscles. B
Exam Question
Explain how the lateral cord integrates multi-segmental ventral motor pools into a coordinated flexor system, and analyze how its anatomical formation, functional organization, and branch distribution determine the pattern of motor deficits observed in lateral cord lesions.
Lateral Pectoral Nerve
The lateral pectoral nerve is a pure somatic motor (GSE) branch of the brachial plexus, arising from the lateral cord (C5–C7). It courses anteriorly, typically piercing the clavipectoral fascia, to supply predominantly the pectoralis major, especially its clavicular head, and frequently communicates with the medial pectoral nerve via the ansa pectoralis, forming a functional neural network to the pectoral musculature.
At a systems level, the nerve transmits upper-segment ventral motor pool output into the anterior thoracoappendicular musculature. These fibers have already undergone segmental recombination and functional sorting, and are now directed toward muscles responsible for force generation and stabilization at the shoulder–trunk interface. Thus, the lateral pectoral nerve does not act in isolation but as part of a coordinated ventral system integrating trunk and upper-limb mechanics.
Functionally, it contributes to shoulder flexion, adduction, and medial rotation, while playing a critical role in anterior stabilization of the shoulder girdle. Activation of pectoralis major allows effective force transmission from the axial skeleton to the upper limb, particularly during pushing, lifting, and controlled positioning of the humerus.
Despite its name, the lateral pectoral nerve does not define a “lateral” muscular territory, but rather reflects its origin from the lateral cord. Its frequent communication with the medial pectoral nerve ensures functional redundancy and coordinated activation of the pectoral muscles, allowing smooth and graded motor output.
Clinically, isolated injury is uncommon and typically results in subtle weakness of shoulder flexion and adduction, particularly in movements heavily dependent on pectoralis major. However, due to dual innervation via the medial pectoral nerve, deficits are often partial rather than complete, illustrating the principle of overlapping innervation within proximal muscle groups.
In summary, the lateral pectoral nerve transmitting integrated motor output to the pectoralis major to enable shoulder girdle stabilization, force transmission, and coordinated upper-limb positioning.
Exam Question
Analyze the role of the lateral pectoral nerve in integrating upper plexus motor output into shoulder girdle mechanics, and explain how its communication with the medial pectoral nerve contributes to functional redundancy and the partial preservation of function following injury.
Musculocutaneous Nerve
The musculocutaneous nerve is a mixed peripheral nerve of the brachial plexus arising from the lateral cord (C5–C7), containing:
GSE (general somatic efferent) – motor to anterior arm musculature
GSA (general somatic afferent) – sensory from lateral forearm
It originates in the axilla, characteristically pierces coracobrachialis, and descends between biceps brachii and brachialis, supplying these muscles before continuing distally as the lateral cutaneous nerve of the forearm.
At a systems level, the nerve represents a terminal ventral-system output, carrying integrated multi-segmental fibers that have undergone recombination (trunks) and functional sorting (divisions). These fibers form a flexion–supination motor pool, coordinating movement across the shoulder, elbow, and forearm within a single functional pathway.
Functionally, it is the primary nerve of the anterior compartment of the arm, mediating:
Elbow flexion (brachialis – primary flexor)
Forearm supination (biceps brachii – powerful supinator)
Shoulder flexion and limb positioning (coracobrachialis, biceps contribution)
Its sensory continuation (GSA) supplies the lateral forearm, linking motor output with a defined cutaneous territory, consistent with the organization of terminal peripheral nerves.
Clinically, injury produces weak elbow flexion and supination with sensory loss over the lateral forearm. However, these actions are not abolished due to functional overlap with radial nerve–supplied muscles (brachioradialis for flexion, supinator for supination), illustrating redundancy within distributed motor pools.
In summary, the musculocutaneous nerve is a mixed terminal nerve, transmitting integrated C5–C7 ventral-system output to the anterior arm, coordinating flexion-supination mechanics while maintaining a coupled sensory distribution.
Exam Question
Explain how the fiber composition (GSE and GSA) and motor distribution of the musculocutaneous nerve determine its functional role, and analyze why its injury results in weakened but preserved flexion and supination in the context of overlapping motor innervation.
Lateral Root of Median Nerve
The lateral root of the median nerve is a fiber-contributing (non-terminal) branch of the brachial plexus arising from the lateral cord (C5–C7), containing:
GSE (general somatic efferent) – motor fibers destined for flexor musculature via the median nerve
GSA (general somatic afferent) – sensory fibers conveyed distally through the median nerve
It courses medially across the axilla to join the medial root (C8–T1) anterior to the axillary artery, forming the median nerve. As an independent structure, it has no direct motor or sensory distribution, functioning instead as a proximal conduction pathway transmitting upper-segment fibers into a composite terminal nerve.
At a systems level, the lateral root represents an essential component of plexus assembly architecture, in which multi-segmental fibers that have already undergone recombination (trunks) and functional sorting (divisions) are redistributed into terminal nerve pathways. It specifically conveys C5–C7 ventral-system motor pools, integrating proximal flexor control with distal forearm and hand function via the median nerve.
Functionally, its significance lies not in independent action but in enabling the median nerve to achieve broad segmental composition and functional capacity. Through this contribution, it supports forearm flexion, wrist and finger flexion, pronation, thenar activity, and precision grip, particularly influencing muscles with strong C6–C7 representation. Thus, it serves as a structural conduit linking proximal integration with distal execution.
Clinically, isolated lesions of the lateral root are rare but may selectively impair the upper-segment contribution to the median nerve, leading to partial weakness of proximal median-innervated functions while sparing components supplied predominantly by C8- T1 via the medial root.
In summary, the lateral root of the median nerve is a non-terminal integrative conduit, transmitting C5–C7 ventral motor and sensory fibers into the median nerve, playing a critical role in the multi-segmental construction and functional capacity of a major terminal pathway.
Exam Question
Explain why the lateral root of the median nerve is best understood as a conduction pathway rather than an independent nerve, and analyze how its fiber composition and contribution to median nerve formation influence the clinical pattern of proximal median nerve dysfunction.
MEDIAL CORD
Description
AI-Generated Illustration-MyoAntomy
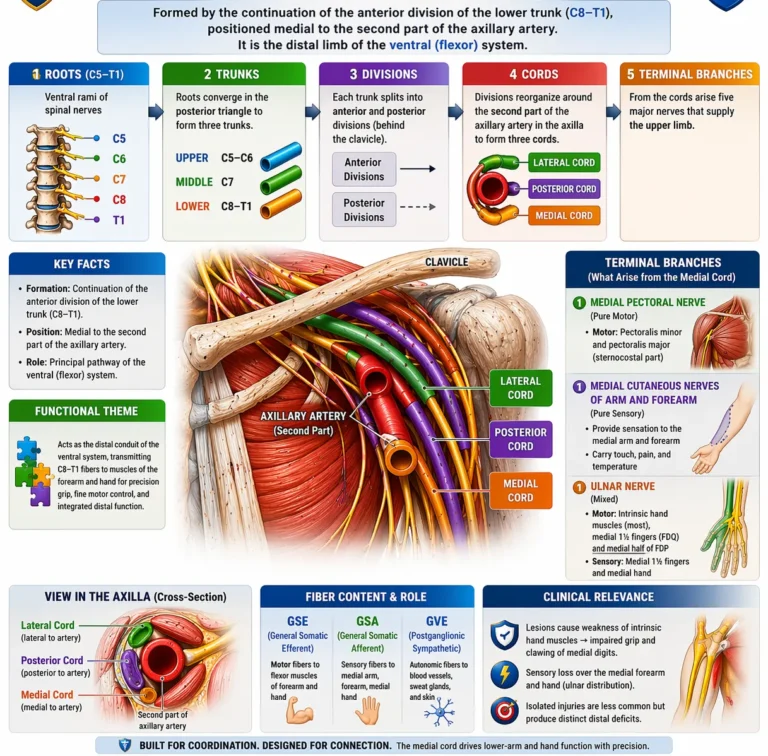
The medial cord of the brachial plexus is the continuation of the anterior division of the lower trunk (C8–Th1), positioned medial to the second part of the axillary artery, containing:
GSE (general somatic efferent) – motor fibers to distal flexor and intrinsic hand musculature
GSA (general somatic afferent) – sensory fibers to the medial upper limb
GVE (postganglionic sympathetic) – autonomic fibers to vascular and cutaneous targets
It represents the distal specialization of the ventral (flexor) system, conveying fibers that have undergone both segmental recombination (trunks) and functional sorting (divisions), now organized into pathways dedicated to fine motor control and precision manipulation.
At a systems level, the medial cord transmits lower-segment motor pools (C8–T1), which are intrinsically biased toward distal musculature, particularly the intrinsic muscles of the hand. This reflects the somatotopic organization of the ventral horn, where neurons controlling distal, high-precision movements occupy more lateral positions and are capable of fractionated, independent motor output. Consequently, the medial cord is functionally linked to dexterity, grip modulation, and coordinated finger movement.
Functionally, it serves as the principal pathway for:
Intrinsic hand function (predominantly via the ulnar nerve)
Distal forearm flexion and fine control
Precision grip and coordinated digital activity
Its branches – the medial pectoral nerve, medial cutaneous nerves of arm and forearm, ulnar nerve, and medial root of the median nerve – demonstrate dual roles: proximal contributions to girdle stabilization and force transmission, and dominant distal contributions to fine motor execution. T
Clinically, medial cord lesions result in loss of intrinsic hand function, impaired grip strength, and sensory loss over the medial aspect of the limb. Because these fibers underlie fine motor control, deficits are disproportionately severe, with marked impairment of precision tasks despite relative preservation of proximal movements.
In summary, the medial cord represents the terminal stage of distal ventral-system specialization, channeling C8–Th1 motor and sensory output into pathways responsible for precision, dexterity, and coordinated hand function, forming the neural basis of fine upper-limb control.
Exam Question
Explain how the medial cord embodies distal specialization of ventral motor pools, and analyze how its fiber composition, somatotopic organization, and branch distribution determine the pattern and severity of motor and sensory deficits observed in medial cord lesions.
Medial Pectoral Nerve
The medial pectoral nerve is a pure somatic motor (GSE) branch of the brachial plexus arising from the medial cord (C8–T1), containing:
GSE (general somatic efferent) – motor fibers to pectoral musculature
It typically pierces pectoralis minor and continues to supply pectoralis major (sternocostal portion), often communicating with the lateral pectoral nerve via the ansa pectoralis, forming a coordinated motor network.
At a systems level, the nerve transmits lower-segment ventral motor pool output into the anterior thoracoappendicular musculature. Compared to the lateral pectoral nerve (C5–C7), it contributes more strongly to force-generating and stabilizing functions, reflecting the increasing role of C8–Th1 fibers in powerful, load-bearing movements.
Functionally, it supports:
Scapular stabilization (via pectoralis minor)
Shoulder adduction and medial rotation (via pectoralis major)
Force transmission between trunk and upper limb
Assisted forced inspiration (rib elevation when scapula is fixed)
Clinically, injury may weaken adduction and medial rotation, and impair stabilization of the scapulothoracic interface, but deficits are often partial due to dual innervation via the lateral pectoral nerve. This demonstrates functional redundancy within proximal muscle groups.
In summary, the medial pectoral nerve is a distal ventral-system motor branch, transmitting C8–Th1 output to the pectoral musculature, optimizing stability, force generation, and coordinated trunk–limb mechanics.
Exam Question
Analyze how the medial pectoral nerve contributes to both scapular stabilization and upper-limb force generation, and explain how its segmental origin and communication with the lateral pectoral nerve influence the clinical presentation of its injury.
Medial Cutaneous Nerve
The medial cutaneous nerves of the arm and forearm are pure sensory (GSA) branches of the brachial plexus arising from the medial cord (C8 – T1), containing:
GSA (general somatic afferent) – cutaneous sensory fibers
They provide cutaneous innervation to the medial aspect of the arm and forearm, transmitting sensory modalities including touch, pain, and temperature.
At a systems level, these nerves represent the peripheral sensory expression of lower brachial plexus segments (C8 – T1). Unlike motor branches, they do not participate in force generation but instead maintain continuous sensory mapping of the medial limb, contributing to proprioceptive awareness and protective sensation.
Functionally, they:
Provide continuous cutaneous sensory coverage of the medial limb
Transmit nociceptive and tactile information
Maintain segmental sensory representation within integrated plexus output
Clinically, injury leads to sensory loss over the medial arm and forearm, without motor deficit. Because these are purely sensory pathways, deficits are localized and modality-specific, often used to assess integrity of C8 – T1 contributions within the plexus.
In summary, the medial cutaneous nerves represent the sensory outflow of the medial cord, maintaining cutaneous representation of lower plexus segments and providing essential input for protective and integrative sensory function.
Exam Question
Explain how the medial cutaneous nerves preserve segmental sensory representation within the brachial plexus, and discuss how their fiber composition and distribution contribute to the clinical localization of C8–T1 lesions.
Ulnar nerve
The ulnar nerve is a mixed peripheral nerve of the brachial plexus arising from the medial cord (C8–T1), containing:
GSE (general somatic efferent) – motor fibers to intrinsic hand and select forearm flexors
GSA (general somatic afferent) – sensory fibers to the medial hand and digits
GVE (postganglionic sympathetic) – autonomic fibers to vascular and cutaneous structures
It descends along the medial arm, passes posterior to the medial epicondyle (cubital tunnel), and enters the hand via Guyon’s canal, reflecting key anatomical points of vulnerability.
At a systems level, the ulnar nerve represents the dominant distal output of lower brachial plexus motor pools (C8–Th1), specialized for fine motor control, intrinsic hand coordination, and precision grip modulation. These fibers originate from lateral ventral horn regions responsible for fractionated, high-resolution motor activity, enabling independent finger movement.
Functionally, it supplies:
Forearm: flexor carpi ulnaris, medial half of flexor digitorum profundus → ulnar deviation + distal finger flexion
Hand (intrinsic muscles): interossei, medial lumbricals (3rd & 4th), adductor pollicis, deep head of FPB → finger abduction/adduction, grip strength, precision control
It is therefore the principal nerve of intrinsic hand mechanics, essential for power grip, precision grip, and coordinated digital movement.
Clinically, injury results in:
Loss of interossei → impaired finger abduction/adduction
Weak grip strength
Clawing of medial digits (ulnar claw)
Sensory loss over medial hand (5th and medial 4th digit)
Because intrinsic hand muscles depend heavily on ulnar innervation, deficits are severe and functionally disabling, particularly affecting fine motor tasks.
In summary, the ulnar nerve is the primary executor of distal ventral-system output, translating C8-Th1 motor pools into fine motor control, grip modulation, and coordinated hand function.
Exam Question
Analyze how the ulnar nerve reflects distal specialization of lower brachial plexus motor pools, and explain how its anatomical course and motor distribution account for the characteristic motor and sensory deficits observed in ulnar nerve lesions at different levels.
Medial Root of Media Nerve
The medial root of the median nerve is a fiber-contributing (non-terminal) branch of the brachial plexus arising from the medial cord (C8–T1), containing:
GSE – motor fibers destined for median nerve targets
GSA – sensory fibers conveyed via the median nerve
GVE – postganglionic sympathetic fibers
It courses laterally across the axilla to unite with the lateral root (C5–C7) anterior to the axillary artery, forming the median nerve. As an independent structure, it has no direct motor or sensory distribution, functioning as a distal segment conduit transmitting lower-segment fibers.
At a systems level, it represents the C8–Th1 contribution to the median nerve, complementing the lateral root (C5–C7) to create a fully integrated multi-segmental nerve. This arrangement allows the median nerve to coordinate both proximal flexor function and distal precision control, combining upper and lower motor pool contributions.
Functionally, through the median nerve, these fibers support:
Distal forearm flexion (fine control)
Thenar musculature → thumb opposition and precision grip
Lateral lumbricals → coordinated finger flexion-extension balance
Thus, the medial root is critical for establishing the lower-segment component of precision hand function, even though it has no independent peripheral field.
Clinically, isolated lesions are rare but may selectively disrupt the C8-Th1 contribution to the median nerve, leading to disproportionate impairment of fine motor control and grip precision, while partially sparing functions dominated by C5–C7 fibers.
In summary, the medial root of the median nerve is a distal integrative conduit, transmitting C8–T1 fibers into the median nerve, enabling its role as a multi-segmental, functionally versatile terminal nerve.
Exam Question
Explain how the medial root contributes to the multi-segmental organization of the median nerve, and analyze how disruption of this component affects the balance between proximal flexor function and distal precision control in the upper limb.
POSTERIOR CORD
Description
AI-Generated Illustration-MyoAntomy
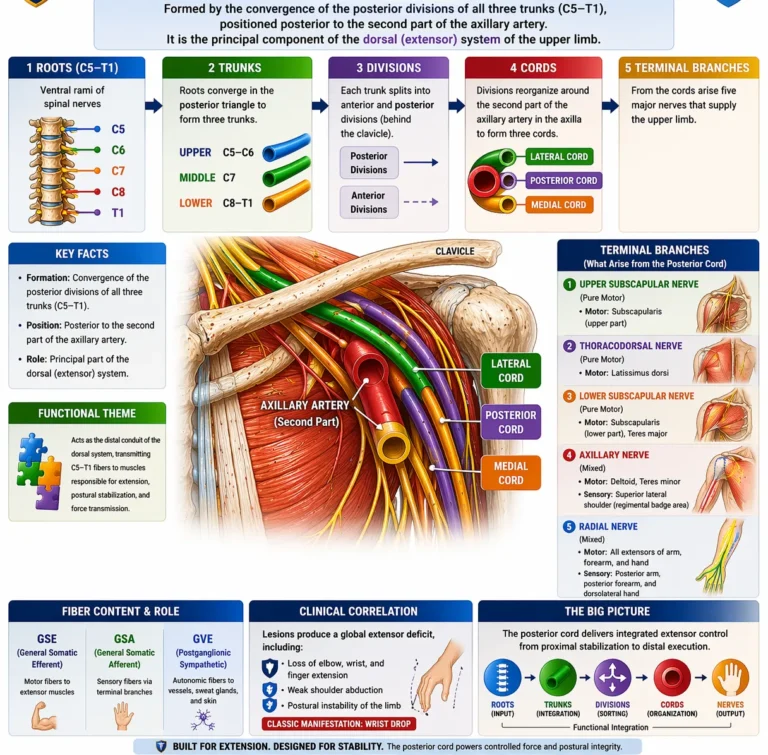
The posterior cord of the brachial plexus is formed by the convergence of the posterior divisions of all three trunks (C5–Th1) and is positioned posterior to the second part of the axillary artery, containing:
GSE (general somatic efferent) – motor fibers to extensor musculature
GSA (general somatic afferent) – sensory fibers conveyed via terminal branches
GVE (postganglionic sympathetic) – autonomic fibers to vascular and cutaneous targets
It represents the dorsal (extensor) system of the upper limb, carrying fibers that have undergone both segmental recombination (trunks) and functional sorting (divisions), now organized into a unified pathway for extension, abduction, and postural stabilization.
At a systems level, the posterior cord integrates multi-segmental dorsal motor pools (C5–Th1) derived from the dorsal embryological muscle mass. These fibers are specialized for powerful, coordinated extension across multiple joints, enabling the limb to generate force, maintain posture, and counterbalance flexor activity. This reflects the fundamental biomechanical role of extensors in load-bearing, anti-gravity stabilization, and controlled limb positioning.
Functionally, it serves as the principal pathway for:
Shoulder abduction and stabilization (via axillary nerve)
Arm, forearm, wrist, and finger extension (via radial nerve)
Posterior shoulder girdle and axial force transmission (via subscapular and thoracodorsal branches)
Its major branches – including the axillary nerve, radial nerve, upper and lower subscapular nerves, and thoracodorsal nerve – demonstrate a continuum from proximal stabilization (scapular control) to distal extension mechanics, forming a coordinated extensor network.
Clinically, lesions of the posterior cord produce global extensor deficits, including loss of shoulder abduction, elbow extension, and wrist/finger extension, often manifesting as wrist drop. Because the cord contains fibers from all spinal levels (C5–Th1), deficits are broad and multi-joint, reflecting disruption of an entire functional system rather than a single segment or nerve.
In summary, the posterior cord represents the integrated dorsal-system output, channeling multi-segmental motor pools into pathways responsible for extension, postural control, and coordinated anti-gravity function of the upper limb.
Exam Question
Explain how the posterior cord integrates dorsal motor pools into a unified extensor system, and analyze how its anatomical formation and branch distribution account for the widespread motor deficits observed in posterior cord lesions.
Upper Scapular Nerve
The upper subscapular nerve is a pure somatic motor (GSE) branch of the brachial plexus arising from the posterior cord (C5–C6), containing:
GSE (general somatic efferent) – motor fibers to scapular stabilizing musculature
It supplies the upper portion of subscapularis, a key component of the rotator cuff, transmitting dorsal-system motor output to the anterior surface of the scapula.
At a systems level, this nerve conveys proximal dorsal motor pool activity into muscles responsible for glenohumeral stabilization and controlled internal rotation.
Subscapularis functions as both a dynamic stabilizer of the humeral head and a contributor to medial rotation, counterbalancing external rotators and maintaining joint congruency during movement.
Functionally, it supports:
medial (internal) rotation of the humerus
dynamic stabilization of the glenohumeral joint
maintenance of humeral head alignment during motion
This reflects a key principle: proximal posterior cord branches prioritize joint stability and precision control, forming the biomechanical foundation for larger distal movements.
Clinically, isolated injury is uncommon but may subtly impair medial rotation strength and compromise rotator cuff stability, potentially contributing to anterior shoulder instability or altered movement patterns. Deficits are often masked by synergistic muscles (pectoralis major, latissimus dorsi).
In summary, the upper subscapular nerve is a proximal dorsal-system stabilizing branch, transmitting C5–C6 motor output to subscapularis, ensuring joint integrity and controlled rotational movement.
Exam Question
Explain how the upper subscapular nerve contributes to glenohumeral stability, and analyze how its motor supply to subscapularis integrates with other rotator cuff muscles to maintain dynamic joint alignment during upper-limb movement.
Thoracodorsal nerve
The thoracodorsal nerve is a pure somatic motor (GSE) branch of the brachial plexus arising from the posterior cord (C6–C8), containing:
GSE (general somatic efferent) – motor fibers to latissimus dorsi
It descends along the posterior axillary wall to supply the latissimus dorsi, a large superficial muscle linking the upper limb to the axial skeleton.
At a systems level, the thoracodorsal nerve transmits integrated dorsal motor pool output into a muscle specialized for powerful extension, adduction, and internal rotation of the humerus, as well as force transmission between trunk and upper limb.
Latissimus dorsi acts as a major posterior kinetic driver, enabling large-scale movements such as pulling, climbing, and lifting.
Functionally, it supports:
shoulder extension
shoulder adduction
medial rotation of the humerus
powerful pulling and load-bearing actions
It plays a critical role in closed-chain movements, where the upper limb is fixed and the body moves relative to it (e.g., climbing), emphasizing its role in functional integration of trunk and limb mechanics.
Clinically, injury leads to weakness in extension and adduction of the arm, particularly noticeable in activities requiring forceful pulling or climbing. However, deficits may be partially compensated by teres major and posterior deltoid. The nerve is clinically important in axillary surgery, where it may be at risk.
In summary, the thoracodorsal nerve is a major dorsal-system efferent pathway, delivering multi-segmental motor output to latissimus dorsi, enabling powerful, coordinated upper-limb movements and trunk–limb integration.
Exam Question
Analyze the role of the thoracodorsal nerve in integrating upper-limb movement with trunk mechanics, and explain how its motor supply to latissimus dorsi contributes to both open-chain and closed-chain functional activities, including the clinical consequences of its injury.
Lower Subscapular Nerve
The lower subscapular nerve is a pure somatic motor (GSE) branch of the brachial plexus arising from the posterior cord (C5–C6), containing:
GSE (general somatic efferent) – motor fibers to posterior shoulder musculature
It supplies the inferior portion of subscapularis and teres major, transmitting dorsal-system motor output to muscles involved in powerful medial rotation and adduction of the humerus.
At a systems level, this nerve conveys integrated dorsal motor pools into muscles that bridge stabilization and force generation. While subscapularis contributes to dynamic glenohumeral stability, teres major functions as a power generator, assisting in large-scale movements such as pulling and adduction. This reflects a transition from fine joint stabilization (proximal rotator cuff) to forceful limb movement (axial–appendicular integration).
Functionally, it supports:
medial (internal) rotation of the humerus
shoulder adduction
dynamic stabilization of the glenohumeral joint
integration of scapulohumeral mechanics during movement
Clinically, injury may weaken adduction and medial rotation, particularly in actions requiring forceful pulling, but deficits are often partially compensated by latissimus dorsi and pectoralis major. Subtle impairment of joint stability may also occur.
In summary, the lower subscapular nerve is a dorsal-system motor branch, linking stabilizing and force-generating musculature to enable coordinated shoulder movement and power transmission.
Exam Question
Explain how the lower subscapular nerve integrates rotator cuff stabilization with power-generating shoulder movements, and analyze how its muscular distribution influences the clinical presentation of its injury.
Axilary Nerve
The axillary nerve is a mixed terminal branch of the brachial plexus arising from the posterior cord (C5–C6), containing:
GSE (general somatic efferent) – motor fibers to deltoid and teres minor
GSA (general somatic afferent) – sensory fibers to the lateral shoulder (regimental badge area)
GVE (postganglionic sympathetic) – autonomic fibers to local vascular structures
It passes through the quadrangular space with the posterior circumflex humeral artery, wrapping around the surgical neck of the humerus to reach the deltoid region.
At a systems level, the axillary nerve delivers proximal dorsal motor pool output into muscles responsible for shoulder abduction and rotational stability. The deltoid acts as the primary driver of abduction from ~15° to 90°, while teres minor contributes to external (lateral) rotation and joint stabilization. This positions the axillary nerve as a key mediator of glenohumeral biomechanics.
Functionally, it supports:
shoulder abduction (primary driver via deltoid)
lateral rotation (teres minor)
dynamic stabilization of the glenohumeral joint
sensory innervation of lateral shoulder (regimental badge area)
It is essential for elevating and positioning the upper limb, integrating movement with stability.
Clinically, injury (e.g., surgical neck fracture, shoulder dislocation) leads to:
loss of shoulder abduction beyond 15°
flattened deltoid contour (muscle atrophy)
sensory loss over lateral shoulder
Because deltoid is the dominant abductor beyond initiation (supraspinatus), deficits are functionally significant, impairing elevation of the limb.
In summary, the axillary nerve is a proximal mixed terminal nerve, integrating motor and sensory components to enable shoulder abduction, rotational stability, and regional sensation, forming a critical element of upper-limb mobility.
Exam Question
Analyze the role of the axillary nerve in glenohumeral biomechanics, and explain how its anatomical course and fiber composition determine the characteristic motor and sensory deficits observed in surgical neck fractures of the humerus.
Radial Nerve
The radial nerve is a mixed terminal branch of the brachial plexus arising from the posterior cord (C5–T1) and contains
GSE (general somatic efferent) motor fibers
GSA (general somatic afferent) sensory fibers
GVE (postganglionic sympathetic) autonomic fibers.
It is the largest branch of the posterior cord and the principal nerve of the extensor compartments of the upper limb. It conveys integrated multi-segmental fibers to muscles responsible for extension, postural stabilization, and controlled limb positioning.
Anatomically, the nerve leaves the axilla posteriorly, passes through the radial groove of the humerus, and continues toward the lateral elbow, where it divides into a superficial sensory branch and a deep motor branch.
Functionally supplies
the triceps brachii and anconeus in the arm and the extensor-supinator musculature of the forearm. It therefore mediates elbow extension, wrist extension, finger extension, and part of forearm supination, while also stabilizing the upper limb during reaching and release phases of movement. Its action is not limited to producing extension; it establishes the extensor framework against which flexor activity becomes effective.
Its sensory distribution includes the posterior arm, posterior forearm, and dorsolateral aspect of the hand, representing the cutaneous expression of the dorsal upper-limb territory. Through this combined motor and sensory organization, the radial nerve functions as the principal executor of extensor synergy, coordinating proximal force generation with distal release and repositioning.
Clinically, radial nerve injury causes weakness or loss of extension, most characteristically wrist drop, often accompanied by loss of finger extension and reduced grip strength. Sensory loss affects the dorsolateral hand and posterior limb according to lesion level.
In summary, the radial nerve is the dominant dorsal-system terminal nerve, transmitting C5–T1 motor, sensory, and sympathetic fibers into a unified pathway responsible for extension, anti-gravity stabilization, and functional positioning of the upper limb.
Exam Question
Explain why the radial nerve is considered the principal nerve of the dorsal functional system of the upper limb, and analyze how its motor distribution and anatomical course account for the characteristic biomechanical and clinical consequences of radial nerve injury
FUNCTIONAL IMPORTANCE
Motor Integration
The brachial plexus functions as a multisegmental motor integration system (C5–T1), redistributing ventral horn output into peripheral nerves that coordinate muscles across multiple joints.
This allows the upper limb to operate as a linked kinetic chain, where proximal stabilization enables distal mobility through efficient force transmission. Motor output is regulated by descending pathways controlling motor unit recruitment and firing frequency, enabling graded activation from gross proximal movements to fine distal control.
As a result, movements such as reaching, lifting, and manipulation are executed as coordinated, multijoint actions rather than segmental contractions.
Functional Synergy
The plexus organizes fibers into ventral (flexor) and dorsal (extensor) systems, enabling coordinated agonist–antagonist interaction and efficient movement patterns.
This functional sorting allows smooth transitions between movement phases while maintaining joint alignment and mechanical efficiency. Proximal muscles provide stability and force generation, while distal muscles refine movement, allowing simultaneous execution of power and precision.
Thus, the plexus supports integrated actions such as grasping, holding, and releasing through coordinated muscle group activation.
Sensory Integration
The brachial plexus transmits continuous afferent input (touch, pain, temperature, proprioception) from the upper limb, forming a feedback system essential for movement accuracy.
Proprioceptive signals from muscles and tendons regulate position and load, while cutaneous input enables adaptive grip and environmental interaction.
This sensory feedback allows real-time modulation of motor output, ensuring precision, coordination, and mechanical efficiency during dynamic activity.
Reflex Regulation
Through its peripheral pathways, the brachial plexus enables reflex control of muscle tone and joint stability, linking sensory input to rapid motor responses.
Stretch and tension feedback regulate contraction strength and prevent excessive force, while protective reflexes adjust movement under unexpected conditions.
These mechanisms provide automatic stabilization and continuous adjustment, ensuring safe and efficient upper-limb function during both voluntary and load-bearing activities.
CLINICAL RELEVANCE
Upper Plexus Injury
Erb–Duchenne Palsy (C5–C6)
Injury to the superior trunk (C5–C6), typically due to traction between the head and shoulder, disrupts fibers supplying proximal limb musculature (deltoid, supraspinatus, infraspinatus, biceps, brachialis). This results in the classic “waiter’s tip” posture: shoulder adduction and medial rotation, elbow extension, and forearm pronation, reflecting unopposed extensor and pronator activity.
Functionally, there is loss of proximal stabilization and flexor control, impairing shoulder abduction and elbow flexion essential for reaching and lifting. Because fibers are still relatively proximal in the kinetic chain, deficits predominantly affect gross motor function rather than fine control.
Lower Plexus Injury
Klumpke Palsy
Injury to the inferior trunk (C8–T1), often from upward traction of the limb, primarily affects distal motor pools, especially intrinsic hand musculature (ulnar > median distribution). This produces the “claw hand” deformity due to loss of lumbricals and interossei, with unopposed long flexors and extensors.
Associated involvement of T1 sympathetic fibers may result in Horner syndrome (ptosis, miosis, anhidrosis). Functionally, there is severe loss of fine motor control, grip precision, and coordinated finger movement, disproportionately disabling despite preserved proximal strength, reflecting the specialization of distal motor units.
Terminal Nerve Plasy
Terminal nerve lesions represent disruption of fully integrated motor systems, producing deficits that reflect loss of specific biomechanical functions rather than segmental patterns.
Radial nerve palsy (most common)
Typically due to compression in the radial groove (“Saturday night palsy”) or humeral shaft fracture. Results in failure of the extensor system → wrist drop, inability to extend wrist and fingers, impaired grip release. Sensory loss over dorsolateral hand.
Functionally: loss of active limb positioning in space, as extension is essential for hand orientation.
Median nerve palsy
Commonly from carpal tunnel syndrome or forearm injury. Leads to thenar muscle atrophy → ape hand, loss of thumb opposition, impaired precision grip. Sensory loss in lateral 3½ digits.
Functionally: disruption of fine motor control and precision handling, especially pinch and manipulation.
Ulnar nerve palsy
Often due to compression at the elbow (cubital tunnel) or wrist (Guyon’s canal). Causes loss of intrinsic hand muscles → ulnar claw (digits 4–5), impaired finger abduction/adduction, weak grip. Sensory loss in medial 1½ digits.
Functionally: loss of intrinsic hand coordination, severely affecting dexterity.
Compression Syndrome
Compression neuropathies reflect chronic mechanical and ischemic stress on nerves, leading to progressive conduction impairment and eventual structural damage.
Thoracic outlet syndrome → proximal plexus compression → diffuse pain, paresthesia, weakness, possible vascular signs
Carpal tunnel syndrome (median nerve) → most common entrapment neuropathy → numbness, paresthesia, thenar weakness
Cubital tunnel syndrome (ulnar nerve) → intrinsic hand weakness, clawing, sensory loss medial hand
Pathophysiologically, compression first affects large myelinated fibers (motor + proprioceptive) → weakness and coordination loss, followed by sensory disturbance. Chronic cases lead to axon loss and muscle atrophy.