External Surface
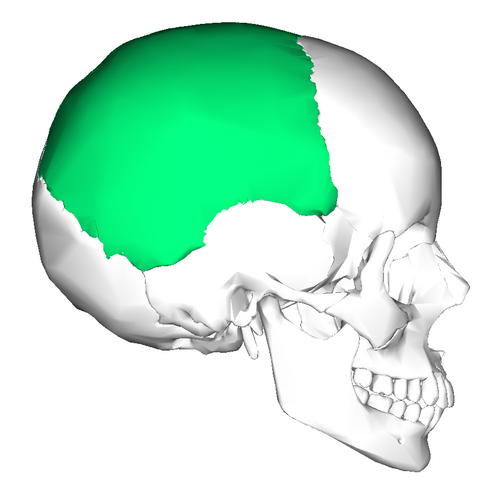
Convex and smooth, forming the outer contour of the skull. The parietal eminence denotes maximal convexity and serves as a key anatomical landmark.
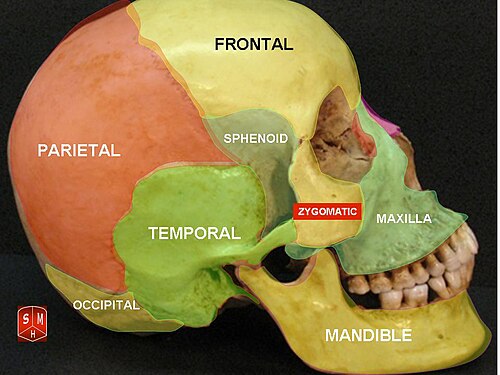
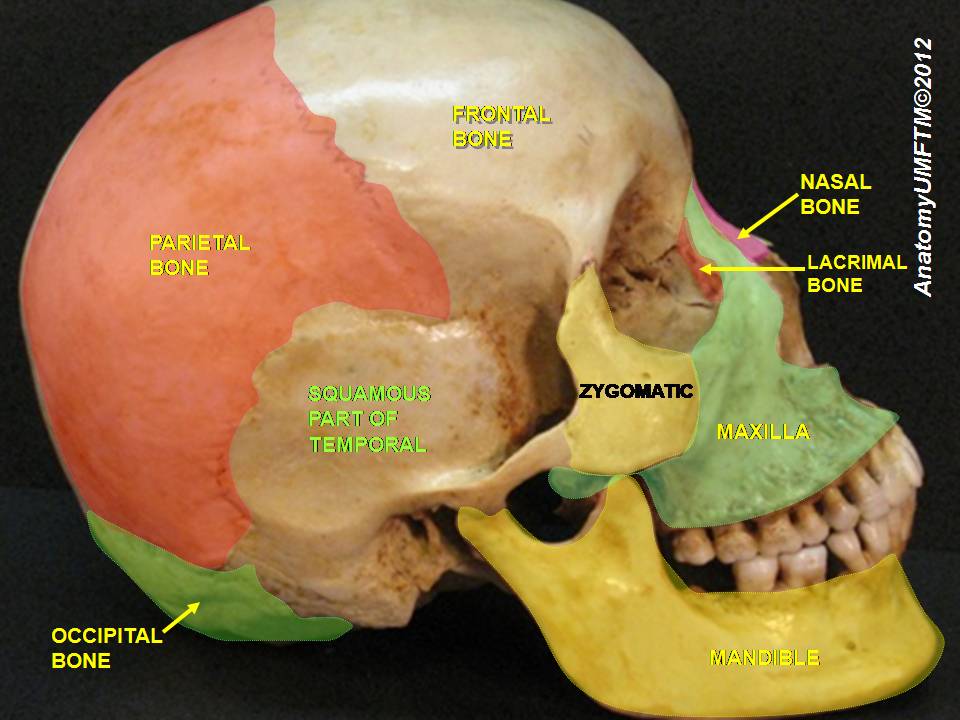
The superior temporal line provides attachment for the temporal fascia, while the inferior temporal line defines the superior boundary of the temporalis muscle origin, linking the parietal bone to masticatory function.
This surface also supports attachment of scalp connective tissues, maintaining structural continuity of the cranial covering.
Internal Surface
Concave, conforming to the cerebral hemispheres, with impressions of cerebral gyri indicating close anatomical relationship.
Distinct arterial grooves reflect the branching pattern of the middle meningeal artery, radiating from the pterional region.
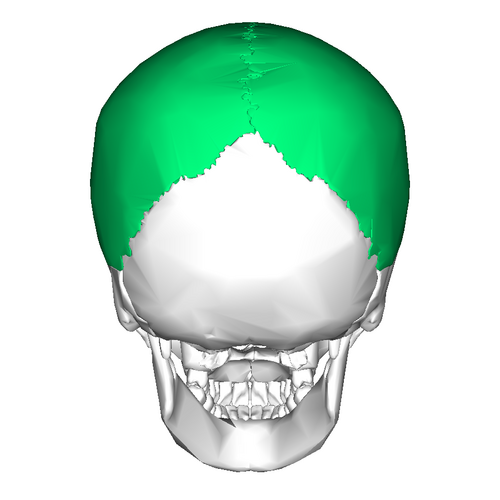
Shallow depressions near the sagittal region correspond to arachnoid granulations, representing sites of cerebrospinal fluid resorption into the superior sagittal sinus.