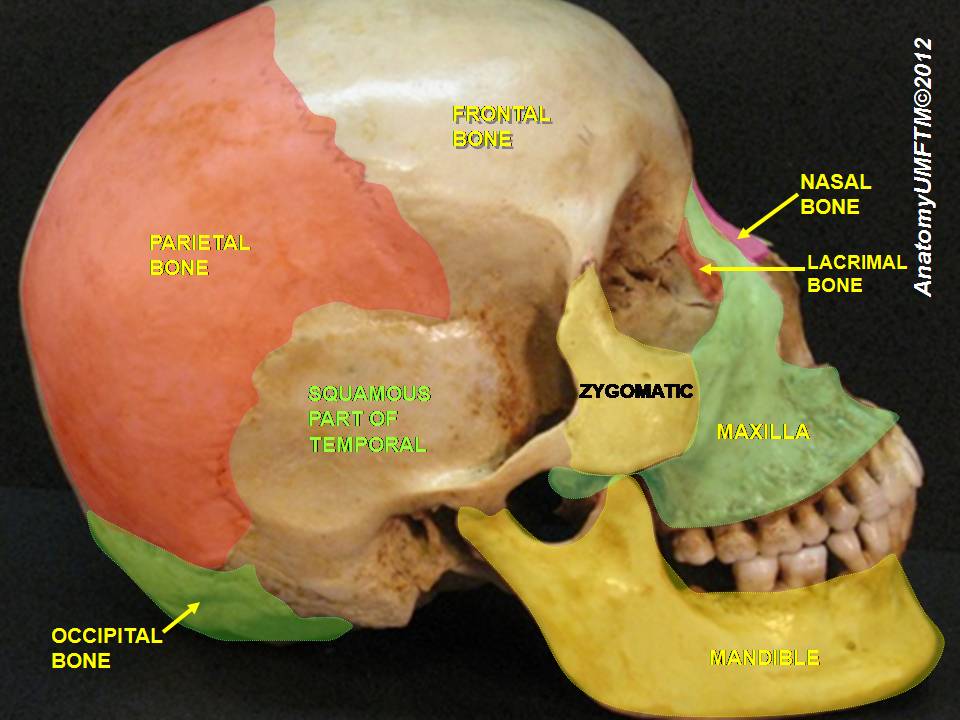
The squamous part is the thin, flat, and superior portion of the temporal bone that forms part of the lateral wall of he cranial vault.
Petrosus Part
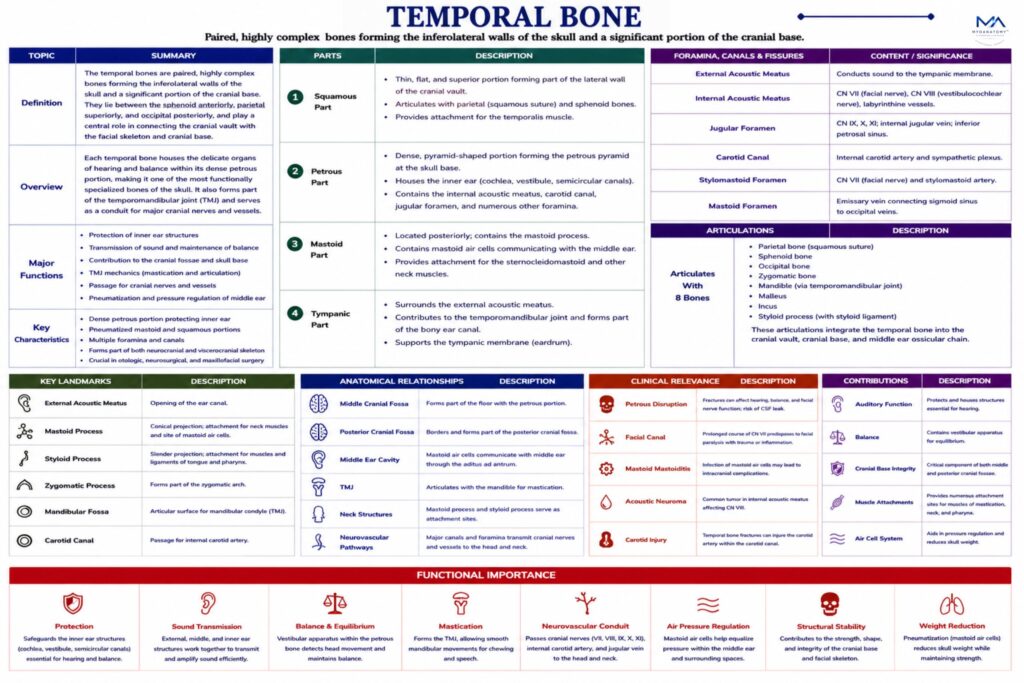
The petrous part is a dense, pyramidal portion of the temporal bone situated at the base of the skull between the sphenoid and occipital bones. It is the hardest bone in the human body due to the protection required for the delicate structures it encloses.
Within the petrous part lie the structures of the inner ear, including:
cochlea (hearing), vestibule (balance), semicircular canals (equilibrium)
major openings
Several important canals and foramina are located within the petrous portion:
Internal acoustic meatus- transmits the facial nerve (CN VII) and the vestibulocochlear nerve (CN VIII) to the inner ear.
Carotid canal-transmits the internal carotid artery, supplying blood to the brain.
Jugular fossa-forms part of the jugular foramen, through which pass:glossopharyngeal nerve (CN IX); vagus nerve (CN X); accessory nerve (CN XI); internal jugular vein
Mastoid Part
The mastoid part lies posterior to the external acoustic meatus and contains the mastoid process, a prominent conical projection that serves as an attachment site for several muscles involved in head movement, including the sternocleidomastoid muscle.
Within the mastoid process are numerous mastoid air cells, which communicate with the middle ear cavity and are lined with mucosa continuous with the middle ear.
These air-filled spaces contribute to
pressure regulation within the middle ear.
Tympanic Part
The tympanic part is a curved plate of bone that surrounds the external acoustic meatus, forming the bony portion of the ear canal.
This region supports the tympanic membrane (eardrum) and forms part of the boundary between the external and middle ear.