Nasal Cavity
MYO CORE

Clinical Relevance
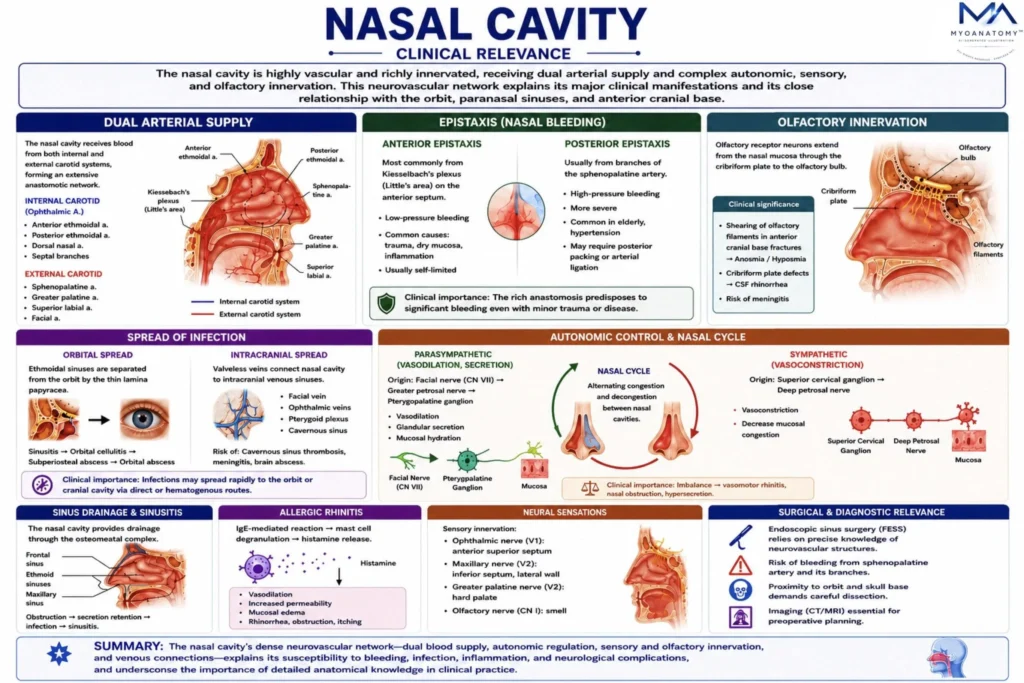
The nasal cavity is a highly specialized neurovascular interface between the external environment and the cranial base. Its mucosa is richly supplied by both the internal and external carotid systems, while its valveless venous drainage communicates with the orbit and intracranial sinuses, creating potential pathways for infection spread.
OVERVIEW
Anatomically, it lies in close relation to the paranasal sinuses, orbit, and anterior cranial fossa. Thin boundaries such as the lamina papyracea and cribriform plate facilitate physiological function but also predispose to orbital and intracranial complications.
Functionally, the nasal cavity regulates airflow, humidification, and immune defense, under complex sensory and autonomic control. This combination of dense vascularity, neural integration, and anatomical connectivity makes it particularly vulnerable to hemorrhagic, infectious, inflammatory, and surgical pathology.
ANATOMY
Epistaxis
The nasal cavity represents one of the most vascularized regions of the body, with dual arterial supply from both the internal and external carotid systems. Epistaxis most commonly arises from the anterior septal region (Kiesselbach’s plexus), where a convergence of ethmoidal, sphenopalatine, greater palatine, and superior labial arteries forms a superficial vascular network.
Anterior epistaxis is typically low-pressure and results from mucosal desiccation, minor trauma, or inflammation. In contrast, posterior epistaxis originates from deeper branches of the sphenopalatine artery, often under higher pressure and associated with significant hemorrhage, particularly in elderly or hypertensive patients.
The anatomical depth and limited accessibility of posterior bleeding sites explain the need for advanced interventions such as posterior packing, endoscopic cauterization, or arterial ligation.
Infection Spread
The nasal cavity is anatomically contiguous with the paranasal sinuses, particularly the ethmoidal air cells, which are separated from the orbit only by the lamina papyracea, an extremely thin bony plate. This structural fragility allows direct spread of infection into the orbital cavity.
Additionally, valveless venous connections between the nasal cavity, pterygoid plexus, and cavernous sinus enable hematogenous dissemination. As a result, untreated infections may progress to orbital cellulitis, subperiosteal abscess, or cavernous sinus thrombosis. This relationship explains why sinusitis – especially ethmoidal – can rapidly become life-threatening, involving cranial nerves and intracranial structures.
Olfactory Loss
Olfactory receptor neurons extend directly from the nasal mucosa through the cribriform plate to the olfactory bulb. This unique arrangement creates a direct anatomical interface between the external environment and the central nervous system.
Trauma to the anterior skull base may shear these delicate fibers, resulting in anosmia. Furthermore, disruption of the cribriform plate can produce cerebrospinal fluid (CSF) rhinorrhea, establishing a direct pathway for pathogens to enter the intracranial compartment.
This makes the region clinically significant in both trauma and infection, with a high risk of ascending meningitis.
Autonomic Control
The nasal mucosa is under precise autonomic regulation. Parasympathetic fibers (via the facial nerve and pterygopalatine ganglion) induce vasodilation and glandular secretion, while sympathetic fibers promote vasoconstriction.
This balance governs the nasal cycle, a physiological alternating congestion-decongestion pattern between the two nasal cavities. Dysregulation leads to pathological conditions such as vasomotor rhinitis, chronic nasal obstruction, and hypersecretion.
Pharmacological agents, including decongestants, exploit this system by inducing sympathetic-mediated vasoconstriction to reduce mucosal edema.
Sinus Drainage
The nasal cavity functions as a central drainage pathway for the paranasal sinuses through the ostiomeatal complex. This region integrates airflow and mucociliary clearance from the maxillary, frontal, and anterior ethmoidal sinuses.
Due to its narrow anatomical configuration, even minimal mucosal swelling can obstruct sinus drainage. This results in secretion retention, impaired ventilation, and subsequent bacterial proliferation, leading to acute or chronic sinusitis.
Thus, obstruction – not infection – is the primary initiating factor in sinus disease.
Venous Spread
Venous drainage of the nasal cavity occurs through a valveless network that communicates with the facial vein, pterygoid plexus, and cavernous sinus. The absence of valves permits bidirectional blood flow, enabling retrograde spread of infection. This anatomical arrangement underlies the clinical concept of the “danger triangle of the face”, where infections of the nasal vestibule or upper lip may propagate intracranially.
Cavernous sinus thrombosis may result, presenting with ophthalmoplegia, cranial nerve deficits, and severe systemic complications.
Allergic Rhinitis
The nasal mucosa contains an extensive immune interface exposed to inhaled antigens. In allergic rhinitis, IgE-mediated hypersensitivity triggers mast cell degranulation, leading to histamine release.
This results in:
vasodilation
increased vascular permeability
mucosal edema
Clinically, this manifests as nasal obstruction, rhinorrhea, and turbinate hypertrophy. Chronic inflammation may alter normal airflow dynamics and predispose to secondary sinus disease.
Surgical Importance
The nasal cavity serves as a primary surgical corridor for endoscopic sinus surgery (FESS) and skull base procedures. Precise anatomical knowledge is essential due to proximity to critical structures, including:
orbit (via lamina papyracea)
anterior cranial fossa (cribriform plate)
major vascular and neural pathways
Iatrogenic injury may result in:
orbital damage
CSF leakage
hemorrhage
Therefore, the nasal cavity represents a high-risk, high-precision surgical region, requiring detailed three-dimensional anatomical understanding.
SUMMARY TABLE