Nasal Cavity
MYO CORE
Neurovascular Supply
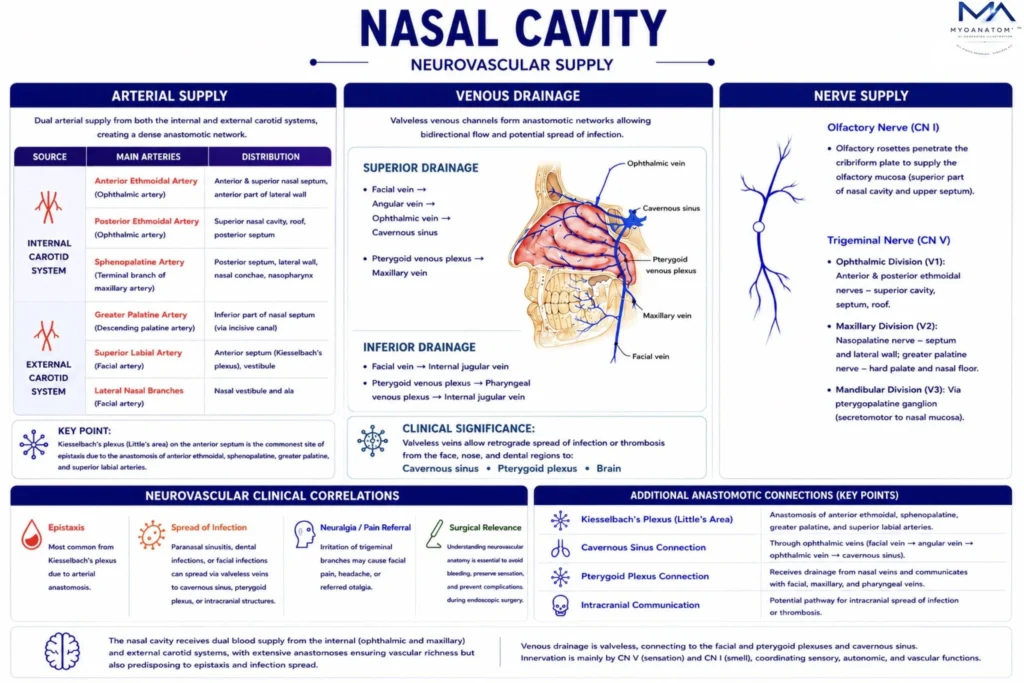
The nasal cavity possesses a specialized neurovascular system essential for respiration, olfaction, mucosal defense, and air conditioning. A dual arterial supply from the internal and external carotid systems forms dense submucosal plexuses that regulate blood flow, optimize warming and humidification of inspired air, and maintain mucosal integrity.
OVERVIEW
Neural supply is similarly complex, combining special sensory (olfactory), general somatic sensory (trigeminal), and autonomic (parasympathetic and sympathetic) components.
These systems regulate sensory perception, glandular secretion, and vascular tone, thereby coordinating airflow dynamics, mucociliary clearance, and reflex responses.
The nasal mucosa also contains an extensive network of venous sinusoids forming erectile tissue, which under autonomic control produces the nasal cycle, an alternating pattern of congestion and decongestion that optimizes respiratory efficiency.
ANATOMY
Arterial System
Arterial supply of the nasal cavity is derived from both the internal carotid system (via the ophthalmic artery) and the external carotid system (via the maxillary and facial arteries), forming a dense and functionally significant anastomotic network within the nasal mucosa.
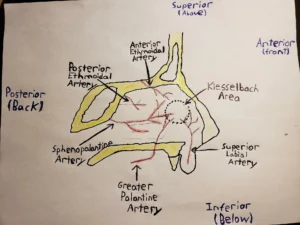
“Kiesselbach’s Plexus” – Mbuchko3, via Wikimedia Commons (2018).
Licensed under CC BY-SA 4.0.
Exam Question
Describe the dual arterial supply of the nasal cavity, specifying its internal and external carotid contributions and the anatomical basis of their mucosal anastomoses.
External Carotid System
Functionally, the external carotid system provides the dominant supply, primarily through the sphenopalatine artery, the terminal branch of the maxillary artery.
Entering the nasal cavity via the sphenopalatine foramen, it divides into posterior septal and posterior lateral nasal branches, supplying the posterior nasal septum and lateral wall. This vascular territory represents the principal perfusion of the nasal cavity and is critically involved in posterior epistaxis.
Additional contributions from the external carotid system include the greater palatine artery, which ascends through the incisive canal to supply the inferior septum, and the superior labial artery, a branch of the facial artery, which supplies the anterior septal region
Exam Question
Identify the branches of the external carotid system supplying the nasal cavity, and explain the anatomical course and dominance of the sphenopalatine artery.
Internal Carotid System
From the internal carotid system, the ophthalmic artery gives rise to the anterior and posterior ethmoidal arteries, which enter the nasal cavity via the ethmoidal foramina.
The anterior ethmoidal artery supplies the anterosuperior septum and lateral wall, while the posterior ethmoidal artery supplies the superior posterior nasal cavity and ethmoidal air cells.
Exam Question
Describe the origin, intracranial course, and nasal distribution of the anterior and posterior ethmoidal arteries.
Arterial Plexuses
These arterial systems converge most prominently in the anteroinferior nasal septum, forming Kiesselbach’s plexus (Little’s area), a highly vascularized arterial anastomotic network involving branches of the anterior ethmoidal, sphenopalatine, greater palatine, and superior labial arteries. This region is the most common site of anterior epistaxis due to its superficial location and high vascular density.
Posteriorly, the nasal cavity is supplied predominantly by branches of the sphenopalatine artery, where vascular structures lie deeper and are often associated with more severe hemorrhage. In this region, vascular contributions are closely related to Woodruff’s plexus, a venous-dominant structure implicated in posterior epistaxis.
Exam Question
Define Kiesselbach’s plexus, detailing its arterial components and explaining its structural predisposition to anterior epistaxis.
Venous Drainage
Venous drainage of the nasal cavity is characterized by a dense, valveless, and highly anastomotic venous network, which permits bidirectional blood flow and creates multiple functional and pathological connections between superficial facial, deep facial, and intracranial venous systems.
This arrangement reflects the dual physiological role of the nasal mucosa in air conditioning and immune defense, while simultaneously conferring a clinically significant risk for the spread of infection.
Exam Question
Characterize the organization of nasal venous drainage, emphasizing the functional and clinical implications of its valveless, anastomotic architecture.
Facial Vein
Anteriorly, venous blood from the nasal cavity drains predominantly into the facial vein via the angular vein, establishing continuity with the superficial venous system of the face. This anterior drainage pathway lies within the region commonly referred to as the “danger triangle of the face”, where venous communications allow retrograde spread of infection toward deeper venous structures.
The absence of valves within these veins enables reversal of flow under conditions of increased intrathoracic pressure or local inflammation.
Exam Question
Outline the anterior venous drainage of the nasal cavity into the facial vein, and explain its relevance to the spread of infection within the facial venous system.
Sphenopalatine Vein
Posteriorly, venous blood is conveyed through the sphenopalatine veins into the pterygoid venous plexus, a complex venous network located within the infratemporal fossa.
The pterygoid plexus serves as a major venous crossroads, receiving blood from the nasal cavity, maxilla, and deep facial regions, and communicating with the maxillary vein, which ultimately contributes to the retromandibular vein.
This plexus also maintains critical connections with intracranial venous sinuses through emissary veins, thereby linking extracranial and intracranial venous circulation.
Exam Question
Describe the posterior venous drainage of the nasal cavity via the sphenopalatine veins and its integration into the deep facial venous network.
Superior Ophthalmic Vein
Superiorly, venous channels from the nasal cavity communicate with the superior ophthalmic vein, which passes through the superior orbital fissure to drain into the cavernous sinus.
This establishes a direct anatomical route between the nasal mucosa and the intracranial venous system. In addition, the pterygoid venous plexus communicates with the cavernous sinus via emissary veins traversing the skull base.
These connections are of major clinical importance, as they provide potential pathways for the spread of infection from the nasal cavity to the cavernous sinus, predisposing to cavernous sinus thrombosis, a life-threatening condition.
Exam Question
Explain the anatomical communication between the nasal cavity and the cavernous sinus via the superior ophthalmic vein.
Pteregoid Venous Plexus
The pterygoid venous plexus is a valveless, highly anastomotic venous network situated within the infratemporal fossa around the pterygoid muscles, functioning as the principal deep venous drainage hub of the midface. It receives blood from the nasal cavity via the sphenopalatine veins, as well as from the maxilla, orbit, and deep facial structures, and drains into the maxillary vein.
Critically, it communicates with the cavernous sinus through emissary veins and with the facial vein via the deep facial vein, establishing a bidirectional pathway between superficial, deep, and intracranial venous systems. Owing to the absence of valves, this plexus permits retrograde flow and constitutes a major route for the spread of infection from the nasal cavity and midface to the cavernous sinus, with significant clinical implications such as cavernous sinus thrombosis.
Exam Question
Describe the anatomical organization and venous connections of the pterygoid venous plexus, and explain its role in facilitating intracranial spread of infection.
Olfactory Innervation
The olfactory region of the nasal cavity, located in the superior nasal concha and adjacent upper septum, is innervated by the olfactory nerve (cranial nerve I). Olfactory receptor neurons within the mucosa project axons through the cribriform plate of the ethmoid bone to synapse in the olfactory bulb. This pathway is highly specialized and clinically vulnerable, particularly in cranial trauma involving the anterior skull base, where disruption may result in anosmia.
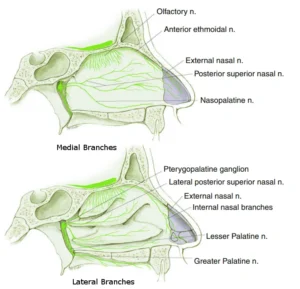
“Posterior Superior Nasal Nerve” – FrozenMan, via Wikimedia Commons.
Licensed under CC BY-SA 4.0.
Exam Question
Describe the anatomical pathway of olfactory nerve fibers from the nasal mucosa to the olfactory bulb, and explain their vulnerability to injury at the cribriform plate.
General Sensory Innervation
General sensory innervation of the nasal cavity is provided by the ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve.
The anterosuperior portion of the nasal cavity is supplied by the anterior ethmoidal nerve, a branch of the nasociliary nerve (V1), which provides sensation to the anterior septum and lateral wall.
The posteroinferior portion is supplied by branches of the maxillary nerve (V2), including the nasopalatine nerve, which innervates the nasal septum, and the posterior superior lateral nasal nerves, which supply the lateral wall.
Inferior regions also receive contributions from the greater palatine nerve.
These sensory pathways mediate touch, pain, and temperature and are involved in protective reflexes, including the sneeze reflex, which serves to clear irritants from the nasal passages
Exam Question
Describe the trigeminal sensory innervation of the nasal cavity, specifying the contributions of V1 and V2 and their regional distribution within the septum and lateral wall.
Autonomic Innervation
Autonomic innervation regulates both vascular tone and glandular secretion within the nasal mucosa.
Parasympathetic fibers, responsible for secretomotor activity, originate from the facial nerve (cranial nerve VII). Preganglionic fibers travel via the greater petrosal nerve, join sympathetic fibers to form the nerve of the pterygoid canal, and synapse in the pterygopalatine ganglion. Postganglionic fibers then distribute along branches of the maxillary nerve to stimulate seromucous glands, increasing mucus secretion and contributing to mucosal hydration.
Sympathetic fibers originate from the superior cervical ganglion and travel via the deep petrosal nerve. These fibers pass through the pterygopalatine ganglion without synapsing and provide vasomotor innervation, producing vasoconstriction of the submucosal venous sinusoids. This reduces mucosal congestion and modulates airflow resistance.
The balance between parasympathetic and sympathetic activity underlies the nasal cycle, a physiological process in which alternating vasodilation and vasoconstriction regulate airflow distribution between the two nasal cavities.
Exam Question
Describe the autonomic innervation of the nasal mucosa, including the origin, course, and functional roles of parasympathetic and sympathetic fibers
SUMMARY TABLE