
Lumbar Plexus
The lumbar plexus is a major component of the peripheral nervous system formed by the ventral rami of spinal nerves L1–L4, often receiving a contribution from the subcostal nerve (T12). It is located within the posterior abdominal wall, embedded in the posterior portion of the psoas major muscle, where the lumbar spinal nerves converge and redistribute before emerging as peripheral nerves.
Anatomically, the plexus forms within the substance of the psoas major, where the ventral rami divide into ascending and descending branches that recombine to form terminal nerves. These branches emerge from the lateral border, medial border, or anterior surface of the psoas major muscle, allowing the plexus to distribute neural fibers to both the abdominal wall and the lower limb.
Functionally, the lumbar plexus provides motor and sensory innervation to the anterior abdominal wall, external genital region, and the anterior and medial compartments of the thigh. Through these connections, it plays a crucial role in locomotion, postural stabilization, and coordinated lower limb movement, particularly during activities involving hip flexion, thigh adduction, and knee extension.
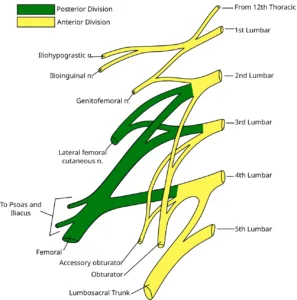
Lumbar Plexus Diagram” – Based on Gray822.svg (Gray’s Anatomy plate), modified by Mcstrother and Ninovolador, via Wikimedia Commons. Licensed under CC BY 3.0
Plexus Branches
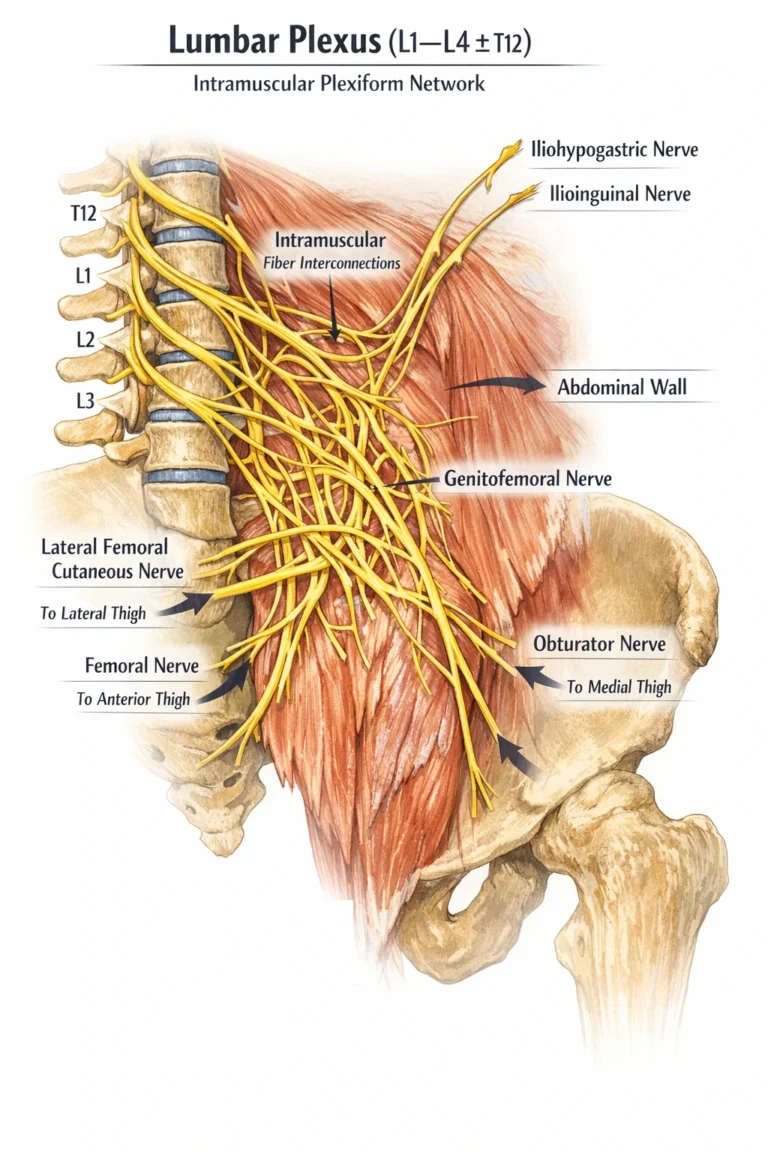
The lumbar plexus is a spatiotemporally organized neural network extending from the lumbar spine into the posterior abdominal wall, formed by the ventral rami of L1–L4 (± T12). Unlike the brachial plexus, it lacks a layered sequence of trunks, divisions, and cords, instead exhibiting a direct intramuscular plexiform organization within the psoas major, where fibers undergo early convergence, splitting, and selective redistribution.
Within the substance of psoas major, segmental fibers interconnect to form a functional network rather than discrete hierarchical levels, with branches emerging at characteristic anatomical borders. Superiorly, short branches (iliohypogastric, ilioinguinal) arise and course toward the abdominal wall, while the genitofemoral nerve emerges anteriorly on the surface of psoas. Laterally, major nerves such as the femoral and lateral femoral cutaneous nerves exit toward the anterior thigh, whereas medially the obturator nerve descends into the pelvis.
This organization reflects a topographically guided redistribution system, in which fibers are arranged according to their target regions rather than through staged structural layers. As a result, terminal branches leave the plexus relatively early, each carrying a multisegmental composition of motor, sensory, and autonomic fibers. These branches extend into the lower abdominal wall and lower limb, enabling coordinated control of hip flexion, knee extension, and thigh adduction, while simultaneously providing integrated somatosensory input and proprioceptive mapping essential for posture and locomotion.
AI-generated illustration ( MyoAnatomy)
Overview
The lateral border of psoas major gives rise to nerves that predominantly supply the anterolateral abdominal wall and anterior thigh, forming the principal flexor–extensor axis of the lower limb and contributing to core stabilization and locomotion. These branches demonstrate a progressive increase in functional complexity, from segmental abdominal wall innervation (L1) to large multijoint motor control (L2–L4).
Illiohypogastric Nerve
The iliohypogastric nerve is a mixed (somatic motor + somatic sensory) branch arising from L1, emerging from the lateral border of psoas major and coursing obliquely across quadratus lumborum, piercing transversus abdominis near the iliac crest.
Motor Innervation:
internal oblique
transversus abdominis
Sensory Innervation:
suprapubic (hypogastric) region
posterolateral gluteal skin
Functional Role:
Maintains abdominal wall tone and integrity
Regulates intra-abdominal pressure(e.g coughing, straining)
Contributes to trunk stabilization and postural control
Clinical Insight:
Represents the upper segment of the thoraco-lumbar neurofunctional continuum, integrating abdominal wall mechanics with pelvic stability.
Ilioinguinal Nevre
The ilioinguinal nerve is a mixed nerve closely associated with the iliohypogastric nerve, following a more inferior course and traversing the inguinal canal to reach the superficial inguinal region.
Motor Innervation:
internal oblique
transversus abdominis (minor contribution)
Sensory Innervation:
upper medial thigh
anterior scrotum(♂) or mons pubis/ (♀)
Functional Role:
Supports lower abdominal wall function, particularly in the inguinal region
Provides somatosensory mapping of the groin and external genitalia
Clinical Insight:
Highly vulnerable in inguinal hernia repair, where injury leads to sensory loss or neuropathic pain.
Lateral Femoral Cutaneous Nevre
The lateral femoral cutaneous nerve is a pure sensory (somatic afferent) branch emerging from the lateral border of psoas major, crossing the iliacus muscle, and passing beneath or through the inguinal ligament near the anterior superior iliac spine (ASIS).
Sensory Innervation:
skin of the lateral thigh
Functional Role:
provides protective cutaneous sensation
Contributes to surface mapping and environmental interaction of the lateral thigh
Clinical Insight:
Compression under the inguinal ligament results in meralgia paresthetica, characterized by burning pain and paresthesia without motor deficit—highlighting its pure sensory nature.
Femoral Nevre
The femoral nerve is the largest and most functionally significant branch of the lumbar plexus, emerging from the lateral border of psoas major and descending between psoas major and iliacus before passing deep to the inguinal ligament into the femoral triangle.
Innervation Type:
Mixed (somatic motor + somatic sensory)
Motor Innervation:
quadriceps femoris → primary knee extensor
iliacus → primary hip flexor (with psoas major)
sartorius → hip flexion, abduction, lateral rotation
pectineus (partial) → hip flexion and adduction
Sensory Innervation:
anterior thigh (anterior cutaneous branches)
medial leg and foot via saphenous nerve
Functional Role:
Knee extension → critical for standing and locomotion
Weight-bearing stability during stance phase
Shock absorption and propulsion during gait
Integrates proximal hip flexion with distal limb control
Insight:
The femoral nerve constitutes the
Overview
The obturator nerve is a mixed (somatic motor + somatic sensory) terminal branch of the lumbar plexus (L2–L4), emerging from the medial border of psoas major and descending along the lateral pelvic wall. It passes through the obturator canal to enter the medial compartment of the thigh, where it typically divides into anterior and posterior branches separated by adductor brevis. Functionally, it represents the principal nerve of the medial (adductor) compartment, forming the coronal plane stabilizing system of the lower limb.
Obturator Nerve
Innervation Type – Somatic motor + somatic sensory
Motor Innevration
adductor longus → primary thigh adduction
adductor brevis → assists adduction and hip flexion
adductor magnus (adductor part) → powerful adduction
gracilis → adduction and knee flexion
obturator externus → lateral rotation and stabilization of the hip joint
Sensory Innervation
skin of the medial thigh (variable distribution)
articular branches to the hip joint and occasionally the knee joint (via subsartorial plexus contribution)
Functional Role
Primary mediator of thigh adduction
Maintains pelvic stability during gait, particularly in single-leg stance
Provides fine control of limb positioning in the coronal plane
Contributes to hip joint stabilization through deep rotators (obturator externus)
Insight
The obturator nerve constitutes the medial stabilizing axis of locomotion, counterbalancing lateral displacement forces generated during walking and running. Through coordinated activation of the adductor group, it ensures controlled limb alignment and energy-efficient gait mechanics, integrating with femoral nerve–mediated anterior compartment activity. Its articular branches further link motor control with proprioceptive feedback, reinforcing joint stability and movement precision.
Overview
The genitofemoral nerve is a mixed (predominantly sensory with focal motor component) branch of the lumbar plexus (L1–L2), emerging on the anterior surface of psoas major, where it descends vertically and divides into genital and femoral branches. Its superficial position reflects its role as an interface between somatic innervation of the thigh and specialized innervation of the inguinal and genital regions, integrating cutaneous sensation with reflex motor function.
Genitofemoral Nerve
Innervation type
Mixed – Somatic sensory + limited somatic motor
genital Branch
Motor: Cremaster muscle (♂)
Sensory: –Anterior scrotum (♂) or/labia majora (♀)
femoral Branch
Sensory only:
Skin of the upper anterior thigh (over femoral triangle)
Functional role
Mediates the cremasteric reflex (L1–L2), linking sensory input from the thigh to motor contraction of the cremaster
Provides somatosensory innervation of the inguinal and proximal femoral region
Integrates lower abdominal wall, inguinal canal, and external genital structures into a unified neurofunctional unit
Insight
The genitofemoral nerve represents a transitional neurofunctional pathway between trunk and limb, combining segmental abdominal innervation (L1) with proximal limb sensory mapping. Its role in the cremasteric reflex illustrates spinal-level integration of sensory and motor circuits, essential for protective and thermoregulatory mechanisms of the testes.
Motor Control
The lumbar plexus provides the principal motor supply to muscles governing hip flexion and knee extension, primarily via the femoral nerve (L2–L4). Activation of the quadriceps femoris enables knee extension and weight-bearing stabilization during the stance phase of gait, while iliopsoas-driven hip flexion advances the limb during the swing phase.
Functional impact: establishes the core biomechanical axis of locomotion and postural support.
Sensory Mapping
Cutaneous branches – including the iliohypogastric, ilioinguinal, genitofemoral, lateral femoral cutaneous, and femoral nerves—provide sensory innervation to the lower abdomen, groin, and thigh. These afferent pathways transmit touch, pain, temperature, and pressure, enabling continuous monitoring of tissue integrity.
Functional impact: supports protective sensation and environmental interaction.
Proprioceptive Integration
Proprioceptive fibers from the hip and knee joints, as well as surrounding musculature, are conveyed through lumbar plexus pathways to the CNS. This input allows real-time assessment of joint position, movement, and mechanical load, forming a feedback loop that refines motor output.
Functional impact: ensures precision, coordination, and adaptive control of lower limb movement.
Gait Dynamics
The lumbar plexus integrates motor and sensory inputs to support dynamic gait cycles, coordinating transitions between stance and swing phases. It maintains upright posture, center-of-gravity control, and efficient energy transfer during walking, running, and climbing.
Functional impact: enables stable, energy-efficient locomotion under varying mechanical demands.
Lumbar Plexopathy
Lumbar plexopathy results from pathology within the posterior abdominal wall (e.g., pelvic trauma, retroperitoneal hemorrhage, tumors, inflammatory neuropathies), disrupting multiple roots (L1–L4) simultaneously. This produces combined deficits in hip flexion, knee extension, and thigh adduction, with sensory loss over the anterior and medial thigh.
Clinical significance: represents failure of a multisegmental neuromuscular network, leading to widespread impairment of locomotion rather than isolated functional loss.
Motor Nerve Injury
Injury to key lumbar plexus branches produces characteristic motor dysfunction:
Femoral nerve (L2–L4): loss of quadriceps function → impaired knee extension, reduced weight-bearing stability, and diminished patellar reflex
Obturator nerve (L2–L4): weakness of thigh adduction, compromising pelvic stabilization
Clinical significance: these deficits disrupt gait mechanics, stance-phase stability, and medial load control, directly impairing efficient movement.
Sensory Neuropathy
The lateral femoral cutaneous nerve is particularly susceptible to compression beneath the inguinal ligament, producing meralgia paresthetica (burning pain, numbness over the lateral thigh).
This reflects a pure sensory neuropathy, illustrating the vulnerability of superficial nerves at anatomical transition zones.
Clinical significance: highlights how selective sensory disruption alters protective feedback and regional perception without affecting motor output.
Surgical Risk
Due to its course within the psoas major and retroperitoneal space, the lumbar plexus is at risk during pelvic/abdominal surgery, hip procedures, and regional anesthesia. Patterns of motor weakness, sensory loss, and reflex changes enable precise localization of lesions within the plexus or its branches.
Clinical significance: disruption compromises balance, gait, and load-bearing capacity, making anatomical knowledge essential for diagnosis, surgical planning, and rehabilitation.
.