
Venous Drainage
Venous drainage constitutes a low-pressure, high-compliance vascular system forming the outflow component of systemic circulation, returning deoxygenated blood and metabolic byproducts from musculoskeletal tissues to the heart. Blood passes from capillaries into postcapillary venules and progressively larger veins, converging into the vena cava and right atrium, thereby determining venous return and influencing cardiac preload and output.
Veins are specialized capacitance vessels with thin walls, reduced smooth muscle and elastic content, and large luminal diameter, allowing substantial volume accommodation with minimal pressure change. Venous valves ensure unidirectional flow, particularly in the limbs.
Within the musculoskeletal system, venous outflow maintains metabolic homeostasis by clearing CO₂, lactate, and H⁺, preserving intracellular pH and sustaining oxidative metabolism.
Venous return is driven by pressure gradients and augmented by the skeletal muscle pump, respiratory dynamics, cardiac suction, and sympathetic venoconstriction.
At the microcirculatory level, venous pressure regulates fluid exchange via Starling forces, maintaining interstitial balance. Functionally, the venous system serves as the principal capacitance reservoir, supporting circulatory homeostasis and continuous capillary exchange.
STRUCTURAL ORGANIZATION
Description
AI-Generated Illustration -MyoAnatomy
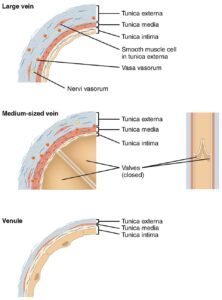
Large Vein, Medium Vein, and Venule (Histological Structure)” – OpenStax College via Wikimedia Commons. Licensed under CC BY 3.0
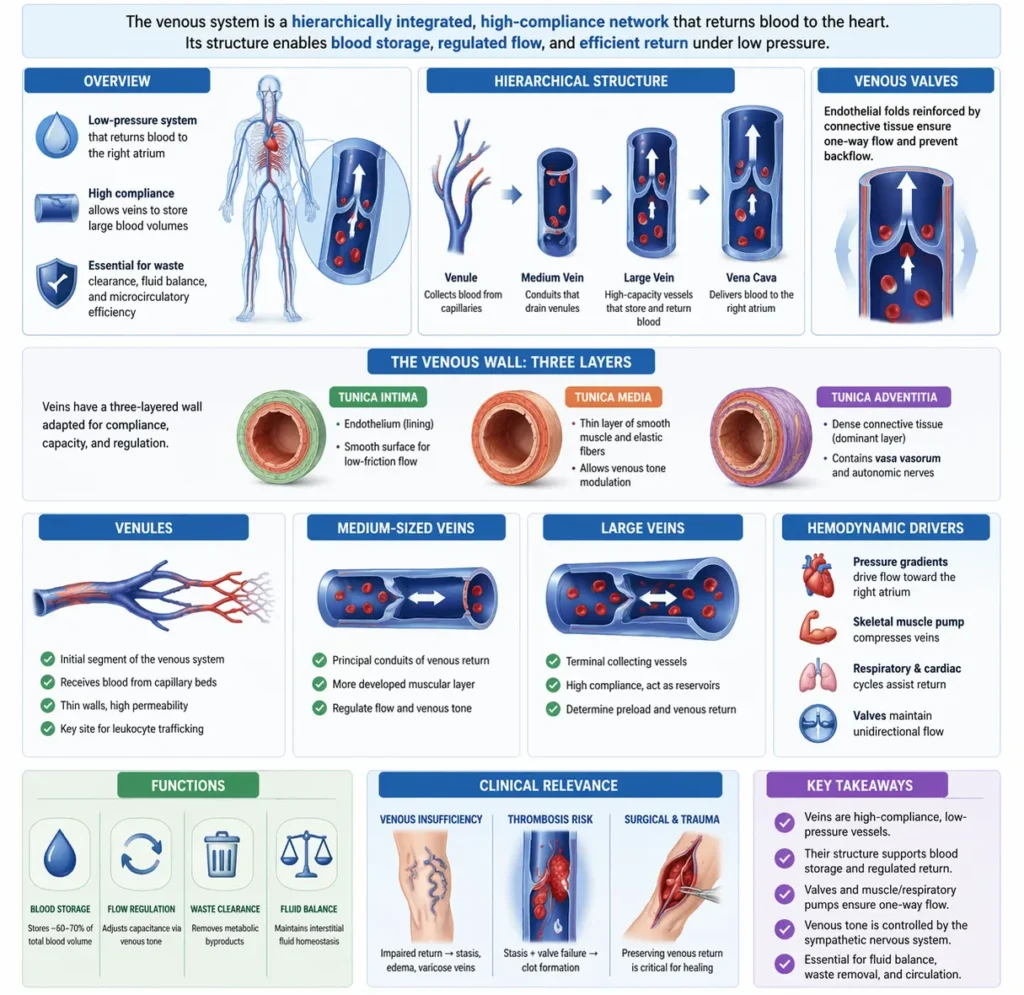
The venous system is organized as a hierarchically integrated, high-compliance vascular network forming the low-pressure outflow component of systemic circulation. It progressively collects blood from capillary beds and returns it to the right atrium, thereby determining venous return, a key determinant of cardiac preload and cardiac output. Within the musculoskeletal system, it is essential for metabolic waste clearance, interstitial fluid regulation, and maintenance of microcirculatory efficiency.
Veins are specialized capacitance vessels capable of accommodating large blood volumes with minimal changes in pressure. This is due to their thin walls, reduced smooth muscle and elastic content within the tunica media, and enlarged luminal diameter. Their high compliance enables dynamic redistribution of blood volume, particularly under sympathetic control.
Despite these adaptations, veins retain a trilaminar structure. The tunica intima consists of an endothelial lining supported by a basal lamina, providing a low-resistance interface and regulating vascular homeostasis via release of nitric oxide, prostacyclin, and anticoagulant factors. It also forms venous valves – endothelial folds reinforced by connective tissue – that ensure unidirectional flow and prevent reflux.
The tunica media is thin, composed of sparse smooth muscle cells and limited elastic fibers, permitting modulation of venous tone through sympathetic (α₁-mediated) venoconstriction, which facilitates central redistribution of blood volume.
The tunica adventitia, typically the dominant layer, consists of dense connective tissue that provides structural support, anchors the vessel, and contains vasa vasorum and autonomic innervation.
Venous vessels are arranged hierarchically from postcapillary venules – key sites of permeability and leukocyte trafficking – to collecting venules, medium veins, and large veins, with increasing connective tissue support as caliber increases.
Hemodynamically, venous return is driven by pressure gradients toward the right atrium and augmented by the skeletal muscle pump, respiratory pressure changes, cardiac suction during diastole, and valve competence. Impairment of these mechanisms leads to venous stasis, elevated hydrostatic pressure, reduced capillary reabsorption, and interstitial fluid accumulation.
At the microcirculatory level, venous pressure critically influences Starling forces, regulating the balance between filtration and reabsorption. Thus, venous structural integrity is essential for maintaining tissue fluid homeostasis, preventing edema, and sustaining cellular metabolism and tissue viability.
Exam Question
Critically analyze how the structural organization of the venous wall, including compliance, valve architecture, and trilaminar composition, supports venous return, and evaluate how dysfunction of these features alters hemodynamics, Starling forces, and tissue fluid balance.
Venules
Venules constitute the initial segment of the venous system, receiving blood directly from capillary beds and forming the primary interface between microcirculation and systemic venous return. Beyond passive drainage, they act as dynamic regulators of microvascular function, critically influencing capillary pressure, permeability, and leukocyte trafficking.
Structurally, venules possess extremely thin walls composed predominantly of endothelial cells with a discontinuous or absent tunica media and minimal connective tissue support. This architecture confers high compliance and permeability, facilitating transendothelial fluid movement and making venules the principal site of leukocyte adhesion via endothelial expression of selectins and integrin ligands during inflammatory activation.
Functionally, venules play a decisive role in modulating Starling forces by influencing downstream venous pressure, thereby regulating the balance between capillary filtration and reabsorption. Within musculoskeletal tissues, their dense distribution enables efficient clearance of metabolites and coordinates inflammatory and reparative responses under conditions of mechanical loading, hypoxia, and tissue injury.
Exam Question
Critically evaluate how the structural and molecular characteristics of venules enable regulation of microvascular permeability, leukocyte extravasation, and Starling forces, and analyze their role in musculoskeletal inflammation and tissue repair.
Medium Size Veins
Medium-sized veins represent the principal conduits of venous return, formed by the convergence of venules and small veins, and are optimized for efficient blood transport under low-pressure conditions while maintaining regulatory capacity over venous tone and flow distribution.
Their trilaminar wall is more developed than in venules, with a modest tunica media composed of circumferential smooth muscle cells capable of α₁-adrenergic–mediated venoconstriction, allowing active modulation of venous capacitance and redistribution of blood volume toward the central circulation. The tunica adventitia, typically the dominant layer, consists of dense collagenous tissue providing structural integrity and anchorage, and contains vasa vasorum and autonomic innervation supporting metabolic and neural regulation.
Venous valves, formed by endothelial folds of the tunica intima reinforced with connective tissue, are a defining feature, particularly in the limbs. These structures maintain unidirectional flow, prevent reflux, and, in conjunction with the skeletal muscle pump, generate segmental pressure gradients necessary for overcoming gravitational forces.
Within the musculoskeletal system, medium-sized veins are integrated within neurovascular bundles, coupling venous return with arterial inflow and neural control. This arrangement enables coordinated regulation of perfusion, supports efficient metabolic exchange, and maintains hemodynamic stability during dynamic changes in posture and muscular activity.
Exam Question
Analyze how the structural organization of medium-sized veins, including smooth muscle-mediated venous tone and valve function, regulates venous return and capacitance, and evaluate their role in maintaining hemodynamic stability and perfusion in the musculoskeletal system under varying physiological conditions.
Large Veins
Large veins represent the terminal collecting vessels of the venous system, integrating blood from multiple peripheral tributaries and directing it toward the right atrium, thereby completing systemic venous return and directly determining cardiac preload. Their function extends beyond passive conduction, acting as major capacitance reservoirs that regulate central blood volume and venous return under varying physiological conditions.
Structurally, large veins are characterized by a relatively thin tunica media and a markedly developed tunica adventitia, which constitutes the dominant layer. The adventitia contains dense collagen fibersand prominent longitudinally arranged smooth muscle bundles, providing tensile strength, preventing overdistension, and facilitating adaptive changes in vessel diameter. This longitudinal smooth muscle organization distinguishes large veins from smaller vessels and contributes to maintenance of vessel patency under low-pressure conditions.
The tunica intima forms a continuous endothelial surface regulating vascular homeostasis, while valve structures are generally absent in central large veins due to proximity to the heart and reduced gravitational constraints. The presence of vasa vasorum and autonomic innervation within the adventitia supports metabolic demands and enables neural modulation of venous tone.
Functionally, large veins operate as dynamic reservoirs with high compliance, capable of storing and mobilizing significant blood volumes in response to sympathetic stimulation. Venoconstriction reduces venous capacitance, increases venous return, and augments cardiac preload, linking venous function directly to cardiac performance.
Hemodynamically, blood flow within large veins is influenced by pressure gradients toward the right atrium, respiratory mechanics, and cardiac suction during diastole. Their large caliber minimizes resistance, allowing efficient, high-volume flow despite low intravascular pressure.
At the systemic level, large veins converge into the superior and inferior vena cava, which deliver venous blood directly to the right atrium, ensuring continuous circulation. Any alteration in compliance, tone, or structural integrity of these vessels significantly impacts central hemodynamics, preload regulation, and overall cardiovascular stability.
Exam Question
Critically evaluate how the structural specialization of large veins, particularly the dominant tunica adventitia and longitudinal smooth muscle organization, supports their role as capacitance vessels, and analyze how alterations in venous compliance and tone influence venous return, cardiac preload, and systemic hemodynamics.
VENOUS RETURN
Description
AI-Generated Illustration-MyoAnatomy
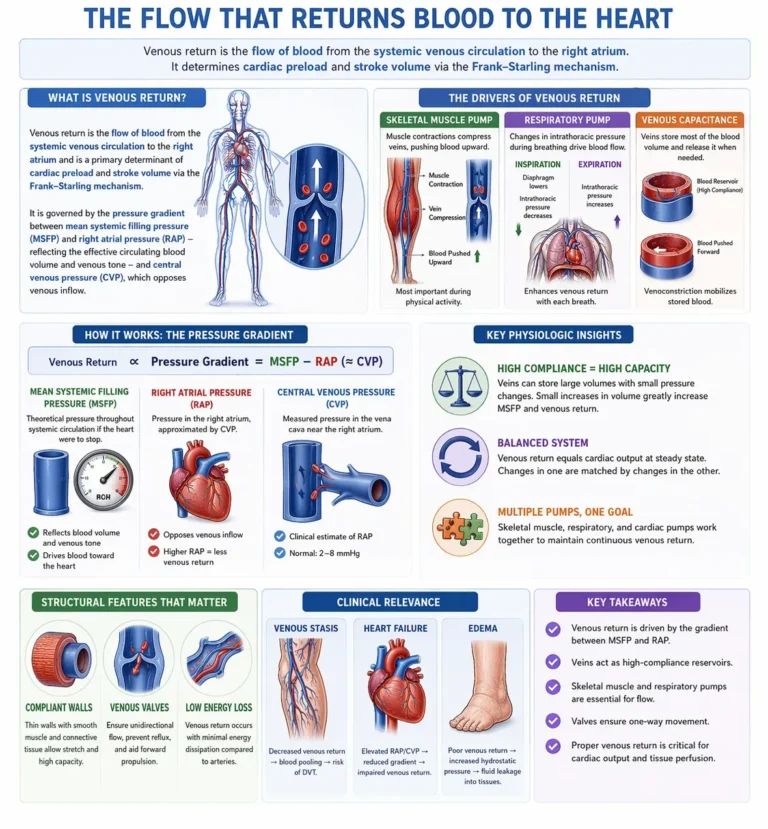
Venous return is the flow of blood from the systemic venous circulation to the right atrium and is a primary determinant of cardiac preload and stroke volume via the Frank–Starling mechanism. It is governed by the pressure gradient between mean systemic filling pressure (MSFP) – reflecting the effective circulating blood volume and venous tone – and right atrial pressure (central venous pressure, CVP), which opposes venous inflow.
Veins function as high-compliance capacitance vessels, capable of storing large blood volumes and dynamically modulating venous return. Sympathetic venoconstriction reduces venous capacitance, elevates MSFP, and enhances the pressure gradient driving blood toward the heart, whereas increased CVP impairs return.
Structural features, including compliant vessel walls and venous valves, ensure unidirectional flow and minimize energy dissipation. Venous return is therefore a dynamically regulated parameter integrating vascular tone, blood volume, and cardiac function to maintain circulatory equilibrium.
Exam Question
Critically analyze the determinants of venous return, incorporating the roles of mean systemic filling pressure, central venous pressure, and venous compliance, and evaluate how their interaction governs cardiac preload and systemic hemodynamics
Skeletal Muscle Pump
The skeletal muscle pump is a dominant extrinsic mechanism enhancing venous return, particularly in the lower limbs. Rhythmic contraction of skeletal muscles compresses deep veins within fascial compartments, generating transient increases in venous pressure that propel blood proximally.
Venous valves partition the blood column, preventing retrograde flow and converting intermittent compression into efficient unidirectional propulsion. This mechanism significantly augments venous return during locomotion and reduces venous pooling.
Functionally, the muscle pump increases effective MSFP locally and improves the pressure gradient toward the heart. Its failure, as in prolonged immobility, results in venous stasis, elevated venous pressure, and increased risk of thrombosis, demonstrating its critical role in both physiology and pathophysiology.
Exam Question
Explain how the skeletal muscle pump modifies local venous pressures and mean systemic filling pressure, and evaluate its role in maintaining venous return and preventing venous stasis under physiological and pathological conditions.
Respiratory Pump
The respiratory pump facilitates venous return through cyclic alterations in intrathoracic and intra-abdominal pressures. During inspiration, diaphragmatic contraction generates negative intrathoracic pressure, lowering right atrial pressure (CVP) and enhancing venous inflow into the thoracic cavity.
Simultaneously, increased intra-abdominal pressure compresses abdominal veins, augmenting upward blood displacement toward the thorax.
During expiration, rising intrathoracic pressure is counterbalanced by venous valves, which prevent retrograde flow and maintain forward movement.
This mechanism enhances the MSFP–CVP gradient and operates synergistically with the skeletal muscle pump and cardiac suction, ensuring continuous venous return under varying physiological states.
Exam Question
Critically evaluate how respiratory-induced pressure changes influence the MSFP–CVP gradient, and explain the interaction between the respiratory pump, venous valves, and cardiac function in maintaining effective venous return..
Starling Forces
Fluid exchange across capillary walls is governed by Starling forces, which determine the net movement of fluid between the intravascular and interstitial compartments. This process reflects a dynamic balance between hydrostatic and oncotic pressures, modulated by capillary permeability and surface area.
Capillary hydrostatic pressure (Pc) promotes filtration by driving fluid outward into the interstitial space, whereas plasma oncotic pressure (πc), generated primarily by albumin, opposes filtration and favors reabsorption. Interstitial hydrostatic (Pi) and oncotic pressures (πi) further influence this balance.
Net fluid movement is described by the Starling equation, integrating these forces along with the filtration coefficient (Kf) and reflection coefficient (σ), which account for capillary permeability and protein restriction:
→ Net filtration ∝ Kf [(Pc − Pi) − σ(πc − πi)]
In most systemic capillary beds, filtration predominates at the arteriolar end, while reduced hydrostatic pressure at the venular end favors reabsorption; however, a significant proportion of filtered fluid is returned via the lymphatic system rather than direct venous reuptake.
At the functional level, venous pressure critically influences capillary hydrostatic pressure; elevations in venous pressure (e.g., venous obstruction or heart failure) increase Pc, shifting the balance toward filtration and promoting interstitial edema.
Thus, Starling forces provide the mechanistic link between microcirculation and venous dynamics, integrating vascular pressure, plasma protein concentration, and lymphatic drainage to maintain tissue fluid homeostasis.
Exam Question
Critically analyze the Starling forces governing capillary fluid exchange, and evaluate how alterations in venous pressure, plasma oncotic pressure, and capillary permeability contribute to the development of edema in pathological states.
Venous Return
Venous return is the flow of blood from the systemic venous circulation to the right atrium and constitutes a primary determinant of cardiac preload and stroke volume via the Frank–Starling mechanism. It is governed by the pressure gradient between mean systemic filling pressure (MSFP) – reflecting effective circulating volume and venous tone – and right atrial pressure (central venous pressure, CVP), which acts as the principal opposing force to venous inflow.
Veins function as high-compliance capacitance vessels, containing the majority of circulating blood volume. Variations in venous tone, mediated predominantly by sympathetic activity, modulate venous capacitance: venoconstriction decreases compliance, elevates MSFP, and enhances venous return, whereas venodilation increases vascular capacity and reduces effective circulating volume.
Venous return is further augmented by extrinsic mechanisms. The skeletal muscle pump generates intermittent increases in venous pressure, propelling blood proximally, while venous valves ensure unidirectional flow and prevent reflux. The respiratory pump enhances return through cyclic pressure gradients: inspiration lowers intrathoracic pressure (reducing CVP) and increases intra-abdominal pressure, thereby facilitating centripetal blood movement.
At the hemodynamic level, venous return is dynamically balanced with cardiac output; under steady-state conditions, both must be equal. Alterations in blood volume, venous compliance, autonomic tone, or right atrial pressure directly shift this equilibrium, influencing preload and systemic perfusion.
Clinically, impaired venous return – due to elevated CVP (e.g., heart failure), reduced muscle pump activity, or venous obstruction – leads to venous stasis, increased capillary hydrostatic pressure, and interstitial edema, highlighting the central role of venous dynamics in both cardiovascular physiology and pathology.
Exam Question
Critically evaluate the determinants of venous return, incorporating mean systemic filling pressure, central venous pressure, venous compliance, and extrinsic pumping mechanisms, and analyze how their interaction regulates cardiac preload and contributes to pathological states such as venous stasis and edema.
FUNCTIONAL IMPORTANCE
Metabolic Clearence
The venous system maintains the biochemical environment of musculoskeletal tissues by removing carbon dioxide, lactate, hydrogen ions, and other metabolic byproducts generated during cellular activity. This clearance preserves concentration gradients necessary for continuous exchange between capillaries and tissues.
By preventing accumulation of metabolic waste, venous outflow supports normal cellular function and maintains acid–base balance. This is particularly important during increased metabolic activity, where efficient removal of byproducts allows sustained muscle function and prevents early fatigue.
Muscle Performance
Venous drainage is closely linked to skeletal muscle performance, especially during contraction when metabolic demand rises. Efficient removal of metabolites helps maintain optimal conditions for muscle contraction and prevents disruption of normal contractile processes.
Through the action of the skeletal muscle pump, venous return also supports arterial inflow by maintaining pressure gradients within the circulation. This ensures continuous oxygen delivery to active muscles, allowing sustained force production, delayed fatigue, and preservation of neuromuscular efficiency.
Fluid Dynamics
Venous circulation plays a key role in regulating microvascular pressure and interstitial fluid balance. By controlling venous pressure, it influences capillary hydrostatic pressure and therefore the movement of fluid between blood vessels and surrounding tissues.
As capacitance vessels, veins help regulate blood volume distribution and maintain effective circulation. When venous drainage is impaired, increased pressure within the venous system shifts fluid into the interstitial space, leading to edema and reduced efficiency of oxygen and nutrient exchange.
Tissue Repair
The venous system contributes to tissue repair by removing inflammatory mediators, cellular debris, and metabolic waste from the interstitial environment. This clearance supports resolution of inflammation and creates favorable conditions for tissue regeneration.
Efficient venous outflow also helps maintain proper circulation, ensuring delivery of oxygen and nutrients required for healing. By supporting recovery and maintaining tissue integrity, venous drainage plays an essential role in adaptation to mechanical stress and restoration of normal function.
CLINICAL RELEVANCE
Venous Stasis
Venous stasis arises from impaired venous flow, typically due to reduced skeletal muscle pump activity, valvular dysfunction, or vascular obstruction. As venous circulation operates under low pressure, it is highly dependent on active flow mechanisms; disruption leads to blood pooling within the venous system.
Stasis promotes activation of coagulation pathways and endothelial dysfunction, forming a key component of Virchow’s triad (stasis, endothelial injury, hypercoagulability). This environment predisposes to thrombus formation, particularly in deep veins of the lower limbs.
Obstruction of venous outflow increases venous and capillary hydrostatic pressure, impairing tissue drainage and promoting interstitial fluid accumulation. Clinically, this manifests as edema, pain, and reduced perfusion efficiency, with the potential for life-threatening complications such as pulmonary embolism if thrombi embolize.
Chronic Venous Insufficiency
Chronic venous insufficiency (CVI) results from sustained venous hypertension, most commonly due to valvular incompetence leading to retrograde blood flow. Loss of valve function disrupts unidirectional flow and causes persistent elevation of venous pressure, particularly in the lower limbs.
Elevated venous pressure is transmitted to the microcirculation, increasing capillary hydrostatic pressure and promoting fluid extravasation into interstitial tissues. Over time, this leads to chronic edema, tissue hypoxia, and inflammatory changes that impair nutrient delivery and waste removal.
Clinically, CVI manifests as skin changes (hyperpigmentation, fibrosis), venous ulceration, and progressive decline in tissue integrity and muscle function. The condition reflects a chronic imbalance between venous return and microvascular exchange, with long-term structural and functional consequences.
Compartment Syndrome
Compartment syndrome is characterized by increased pressure within a closed fascial compartment, initially compromising venous outflow due to the low-pressure nature of the venous system. Impaired venous drainage leads to rapid accumulation of interstitial fluid, further elevating intracompartmental pressure.
This creates a self-perpetuating cycle in which rising pressure progressively reduces perfusion, eventually impairing arterial inflow. The resulting tissue ischemia leads to cellular hypoxia, ATP depletion, and failure of ion homeostasis, culminating in irreversible damage to muscles and nerves if not promptly relieved.
The condition highlights the critical role of venous outflow in maintaining tissue perfusion and demonstrates how venous dysfunction can precede and amplify arterial compromise
Clinical Integration
Venous dysfunction disrupts multiple physiological processes, including metabolic clearance, fluid balance, and effective tissue perfusion. Impaired venous return elevates capillary hydrostatic pressure, alters Starling forces, and promotes interstitial fluid accumulation, leading to edema and reduced efficiency of oxygen and nutrient exchange.
This cascade compromises muscle performance, delays tissue repair, and contributes to progressive functional decline. The close integration between venous outflow, arterial inflow, and microcirculatory exchange underscores the importance of venous physiology in maintaining musculoskeletal homeostasis.
In clinical practice – across orthopedics, vascular medicine, sports medicine, and rehabilitation – understanding venous dynamics is essential for diagnosing circulatory disorders, preventing complications, and optimizing recovery following injury or prolonged immobility.