
Arterial Supply
Arterial supply constitutes a high-pressure, hierarchically organized vascular system forming the inflow component of systemic circulation, delivering oxygen, metabolic substrates, and signaling molecules from the heart to peripheral tissues along pressure gradients.
Blood is ejected from the left ventricle into the aorta and distributed through elastic arteries (pressure buffering via compliance), muscular arteries (regional distribution), and arterioles, which function as primary resistance vessels regulating tissue perfusion and systemic vascular resistance, before reaching capillary exchange networks. Within the musculoskeletal system, arterial perfusion sustains oxidative metabolism, ATP production, and force generation, while supporting protein synthesis, extracellular matrix turnover, and tissue remodeling.
Perfusion is dynamically governed by flow–metabolism coupling (↓O₂, ↑CO₂, ↓pH, adenosine), endothelial signaling (nitric oxide–mediated vasodilation), and autonomic modulation, enabling precise matching of oxygen delivery to metabolic demand. Functionally, arterial circulation operates as a dynamic interface between cardiac output and cellular metabolism, maintaining homeostasis, facilitating thermoregulation, and enabling adaptation to mechanical loading.
STRUCTURAL ORGANIZATION
Description
AI-Generated Illustration -MyoAnatomy
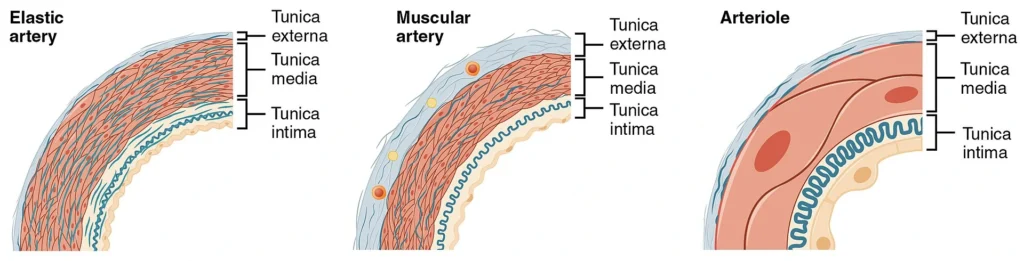
“Muscular and Elastic Artery, Arteriole ( Histological Schematic)” – OpenStax College, via Wikimedia Commons.
Licensed under CC BY 3.0
.
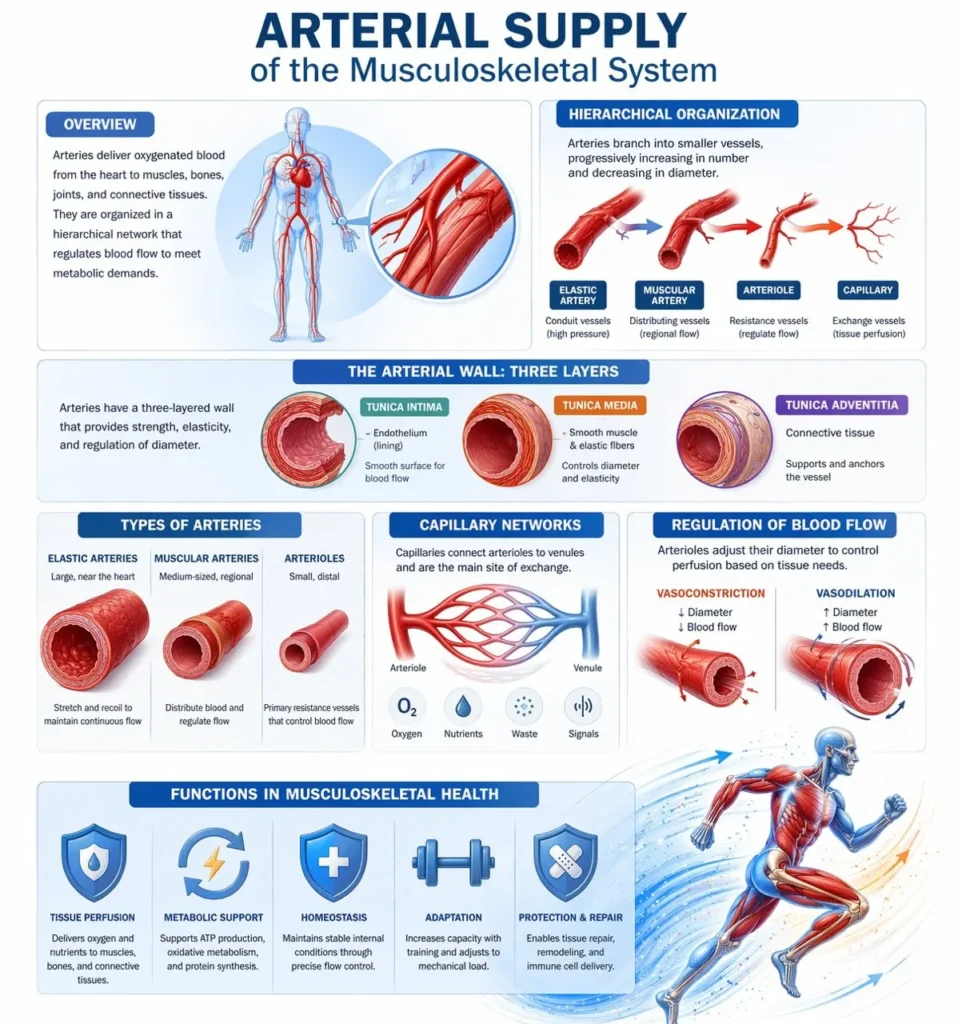
The arterial system forms a hierarchically organized vascular network responsible for transporting oxygenated blood from the heart to peripheral tissues. Structurally and functionally, arteries are classified into several categories according to their diameter, wall composition, and physiological role in regulating blood flow. This organization allows the arterial circulation to efficiently distribute blood throughout the body while maintaining appropriate pressure and perfusion to tissues with varying metabolic demands.
The arterial wall itself typically consists of three concentric layers: the tunica intima, composed of endothelial cells lining the vessel lumen; the tunica media, containing smooth muscle and elastic fibers that regulate vessel diameter; and the tunica adventitia, a connective tissue layer providing structural support and anchoring the vessel to surrounding tissues. Variations in the thickness and composition of these layers account for the functional differences between the major categories of arteries.
Exam Question
How does hierarchical arterial organization- from elastic arteries to arterioles and capillaries – integrate wall structure, vascular resistance, and regional perfusion control to maintain hemodynamic stability and meet the metabolic demands of musculoskeletal tissues?
Elastic Artery
Elastic arteries are large-caliber conducting vessels forming the proximal arterial system, specialized for transforming pulsatile ventricular ejection into continuous flow. Their tunica media contains concentric fenestrated elastic lamellae interspersed with smooth muscle cells, conferring high compliance (ΔV/ΔP) and allowing cyclic energy storage. During systole, vessel expansion stores elastic energy; during diastole, recoil sustains forward flow and maintains diastolic pressure (Windkessel effect), thereby preserving perfusion of high-demand organs such as the myocardium and brain.
Hemodynamically, elastic arteries function as capacitance vessels that attenuate pulse pressure, dampen pulsatile energy transmission, and reduce left ventricular afterload while optimizing distal perfusion. They also modulate pulse wave propagation and reflection, limiting systolic pressure augmentation. Structural integrity depends on elastin-rich extracellular matrix; its degeneration increases arterial stiffness, elevates pulse wave velocity, augments systolic pressure, reduces diastolic pressure, and compromises coronary perfusion.
Endothelial cells regulate vascular homeostasis via shear stress–mediated release of vasoactive mediators (e.g., nitric oxide), while the adventitia contains vasa vasorum supporting the metabolically active vessel wall. Major elastic arteries- including the aorta, pulmonary trunk, common carotid, and subclavian arteries – function collectively as proximal energy reservoirs that stabilize pressure, protect distal microcirculation, and ensure continuous systemic and pulmonary perfusion.
Exam Question
Explain how the structural organization of elastic arteries enables pressure buffering and continuous blood flow, and analyze how changes in arterial compliance influence pulse wave propagation, ventricular afterload, and organ perfusion.
Muscular Artery
Muscular arteries are medium-caliber distributing vessels positioned distal to elastic arteries, specialized for regulating regional blood flow. Their tunica media is composed predominantly of concentric layers of smooth muscle cells with relatively less elastic content, enabling active control of vessel diameter. Through vasoconstriction and vasodilation, they adjust perfusion according to tissue metabolic demand.
Hemodynamically, muscular arteries function as flow-distributing vessels rather than pressure buffers, linking central conducting arteries to peripheral resistance vessels. Changes in vascular radius markedly influence blood flow (flow ∝ r⁴), making them critical regulators of regional perfusion. Their activity is controlled by sympathetic input, circulating hormones, and local metabolic factors, allowing rapid redistribution of blood during physiological states such as exercise and stress
The internal elastic lamina provides structural integrity during repeated diameter changes, while dysfunction of smooth muscle tone contributes to impaired perfusion and increased peripheral resistance, playing a key role in hypertension and ischemic pathology.
Representative muscular arteries – including the brachial, radial, femoral, and tibial arteries –direct blood flow to specific regions, ensuring that tissue perfusion is precisely matched to functional demand.
Exam Question
Explain how the structure of muscular arteries enables regulation of regional blood flow, and analyze how changes in vessel diameter influence perfusion and vascular resistance
Arterioles
Arterioles are the smallest branches of the arterial system and function as the primary resistance vessels regulating blood flow into capillary networks. Their walls consist of a thin tunica media with one to a few layers of smooth muscle cells, yet these cells exert a disproportionate influence on vascular resistance and systemic blood pressure.
Hemodynamically, arterioles are the principal determinants of total peripheral resistance, where small changes in luminal radius produce large changes in flow (flow ∝ r⁴). Through vasoconstriction and vasodilation, they regulate tissue perfusion and redistribute cardiac output according to metabolic demand. Their tone is tightly controlled by sympathetic nervous activity, circulating hormones, and local metabolic factors (e.g., hypoxia, CO₂, H⁺), enabling precise, moment-to-moment regulation of blood flow.
Functionally, arterioles serve as the critical interface between macrocirculation and microcirculation, controlling pressure drop across the vascular system and protecting capillary beds from excessive pressure. Dysregulation of arteriolar tone leads to altered peripheral resistance and is central to the pathophysiology of hypertension, shock, and impaired tissue perfusion
Exam Question
Explain how the structural features of arterioles enable regulation of vascular resistance, and analyze their role in controlling tissue perfusion and systemic blood pressure under varying physiological conditions
Capillaries
Capillaries are the smallest and most numerous vessels, forming the microvascular interface between arterial inflow and venous return and serving as the primary site of exchange between blood and tissues. Structurally, they consist of a single layer of endothelial cells supported by a basement membrane, minimizing diffusion distance and optimizing exchange efficiency.
Functionally, capillaries facilitate the exchange of gases, nutrients, metabolites, and signaling molecules via diffusion, filtration, and transcytosis, governed by concentration gradients and Starling forces. Their organization into capillary beds allows dynamic regulation of flow through precapillary sphincters and local metabolic control, ensuring preferential perfusion of metabolically active tissues.
Within the musculoskeletal system, capillary networks support oxidative metabolism, tissue repair, and adaptation to mechanical load, with capillary density closely correlating with metabolic demand and increasing in response to endurance training. Impairment of capillary function disrupts tissue oxygenation and nutrient delivery, contributing to ischemia and impaired healing.
Exam Question
Describe how the structure of capillaries facilitates exchange between blood and tissues, and evaluate the role of Starling forces and local regulation in determining capillary fluid dynamics and tissue perfusion.
ARTERIAL ANASTOMOSIS
Description
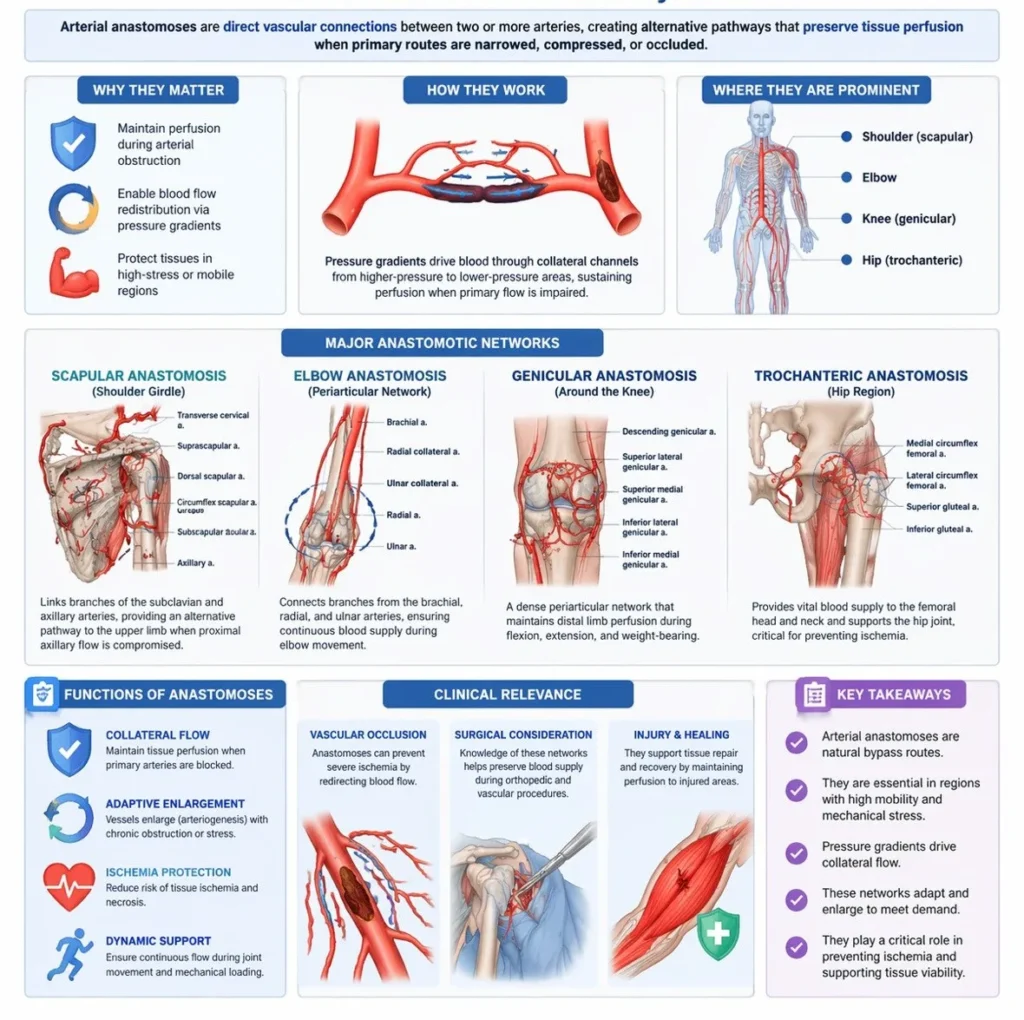
Arterial anastomoses are direct vascular connections between two or more arteries supplying the same anatomical region, forming alternative pathways for blood flow. These networks function as collateral channels that preserve tissue perfusion when the primary arterial route is narrowed, compressed, or occluded.
Hemodynamically, anastomoses enable redistribution of blood flow by allowing pressure gradients to redirect circulation through secondary pathways. In conditions of gradual arterial obstruction, these vessels can undergo adaptive enlargement (arteriogenesis), increasing their capacity to maintain distal perfusion. This collateral circulation is critical in preventing ischemia, particularly in regions exposed to mechanical stress or variable blood supply.
Within the musculoskeletal system, arterial anastomoses are highly developed around mobile joints, where movement may transiently compromise primary vessels. These networks ensure continuous perfusion during changes in joint position and mechanical loading.
Functionally significant anastomotic networks are found around the shoulder (scapular anastomosis), elbow (periarticular arterial network), hip, and knee (genicular anastomosis), where interconnected arterial branches maintain vascular continuity and protect against ischemic injury.
AI-Generated Illustration -MyoAnatomy
Exam Question
Explain the structural and functional significance of arterial anastomoses in maintaining tissue perfusion, and analyze how collateral circulation develops and compensates for arterial occlusion under physiological and pathological conditions.
Scapular
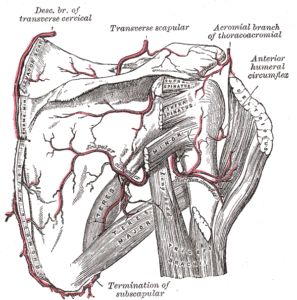
Scapular and Circumflex Arteries (Gray’s Anatomy Plate 521)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
The scapular anastomosis is a collateral arterial network linking branches of the subclavian and axillary arteries, providing an alternative pathway for blood flow to the upper limb when proximal axillary flow is compromised. This network is particularly significant in maintaining perfusion during gradual arterial occlusion or mechanical compression.
Hemodynamically, the scapular anastomosis enables redistribution of blood from the subclavian system to the distal axillary artery via pressure gradients, allowing collateral circulation to sustain limb viability. Over time, these vessels may undergo adaptive enlargement (arteriogenesis), increasing their capacity to compensate for reduced primary arterial flow.
The principal vessels forming this network include the suprascapular artery (from the thyrocervical trunk), the dorsal scapular artery (typically from the subclavian artery), and the circumflex scapular artery (branch of the subscapular artery from the axillary artery). These vessels interconnect within the supraspinous and infraspinous fossae, forming a robust collateral circuit that ensures continuous perfusion of the upper limb.
Exam Question
Explain how the anatomical arrangement of the scapular anastomosis enables collateral circulation between the subclavian and axillary arteries, and analyze its role in maintaining upper limb perfusion during arterial obstruction.
Elbow
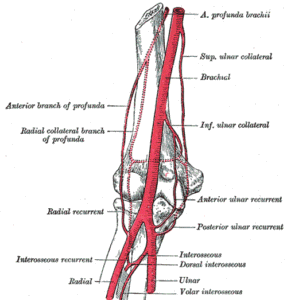
Arteries of the Arm (Gray’s Anatomy Plate 526)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
The elbow anastomosis is a periarticular arterial network formed by descending collateral branches from the brachial artery and ascending recurrent branches from the radial and ulnar arteries, ensuring continuous blood supply around the elbow joint during movement.
Functionally, this network compensates for transient compression or kinking of the main arterial pathways during flexion and extension of the joint, preserving distal perfusion.
Hemodynamically, pressure gradients facilitate redirection of blood through collateral channels, maintaining flow despite positional or mechanical alterations of primary vessels.
Descending collateral arteries include the superior and inferior ulnar collateral arteries and the radial collateral artery (branch of the profunda brachii), while ascending recurrent arteries include the radial recurrent, anterior and posterior ulnar recurrent, and interosseous recurrent arteries. These vessels form a dense periarticular network surrounding the humeroulnar and humeroradial joints, ensuring vascular continuity and protection against ischemia.
Exam Question
Describe the organization of the elbow anastomotic network and analyze how it maintains distal limb perfusion during joint movement and arterial compression.
Genicular
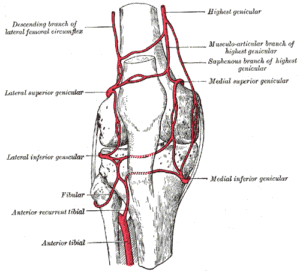
Genicular Anastomosis of the Knee (Gray’s Anatomy Plate 552)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
The genicular anastomosis forms a dense vascular network around the knee joint, maintaining perfusion during joint flexion, extension, and weight-bearing.
The principal arteries forming the genicular network include branches of the popliteal artery, with additional contributions from the femoral and anterior tibial arteries.
Branches of the popliteal artery
Superior medial genicular artery
Superior lateral genicular artery
Inferior medial genicular artery
Inferior lateral genicular artery
Additional contributing arteries
Descending genicular artery – branch of the femoral artery
Descending branch of the lateral circumflex femoral artery
Anterior tibial recurrent artery – branch of the anterior tibial artery
These vessels form a vascular ring surrounding the capsule and ligaments of the knee joint.
Exam Question
Explain how the genicular anastomosis maintains perfusion of the lower limb during knee movement, and analyze its role in compensating for transient or pathological obstruction of the popliteal artery
Other
Trochanteric Anastomosis
The trochanteric anastomosis supplies the femoral head and neck and is particularly important for maintaining the vascular supply of the hip joint.
This arterial network is formed by:
Ascending branch of the medial circumflex femoral artery
Ascending branch of the lateral circumflex femoral artery
Superior gluteal artery
Inferior gluteal artery
These arteries form a vascular ring around the greater trochanter of the femur and contribute to the retinacular arteries supplying the femoral head.
Cruciate Anastomosis
The cruciate anastomosis lies posterior to the proximal femur and connects arteries of the internal iliac system with those of the femoral system.
The arteries involved include:
Medial circumflex femoral artery
Lateral circumflex femoral artery
Inferior gluteal artery
First perforating artery of the profunda femoris
This network provides collateral circulation between the internal iliac and femoral arterial systems.
Exam Question
Explain how periarticular and proximal femoral arterial anastomoses (genicular, trochanteric, and cruciate) function as collateral networks, and analyze their roles in maintaining lower limb perfusion during joint movement, arterial compression, and pathological vascular compromise.
FUNCTIONAL IMPORTANCE
Pulsse Assessment
Arterial pulses represent the propagation of pressure waves through the arterial system and serve as a direct clinical indicator of downstream tissue perfusion. The presence, amplitude, and symmetry of pulses provide essential information about arterial patency, vascular integrity, and overall hemodynamic status.
Clinically, diminished or absent pulses suggest arterial obstruction or ischemia, while asymmetry indicates localized vascular compromise and bounding pulses reflect hyperdynamic circulation. As such, pulse assessment directly correlates with tissue viability, muscular performance, and the capacity for healing within the musculoskeletal system.
Anastomosis
Arterial anastomoses form interconnected vascular networks that provide alternative pathways for blood flow, ensuring continuity of perfusion when primary vessels are compressed or obstructed. This collateral circulation is particularly important in regions of high mobility, such as around joints, where vessels may be transiently occluded during movement.
Functionally, anastomoses maintain consistent blood supply under varying mechanical conditions and enable adaptive redistribution of flow. Clinically, they are critical in gradual arterial occlusion, where collateral compensation can preserve tissue viability; failure of these networks leads to ischemia, necrosis, and loss of function.
Functional Integration
Within the musculoskeletal system, arterial circulation is fundamental for sustaining mechanical performance and structural integrity. By delivering oxygen and metabolic substrates, it supports ATP production required for muscle contraction, facilitates tissue repair and remodeling, and contributes to joint function through synovial and subchondral perfusion. Furthermore, arterial supply enables adaptation to mechanical stress by supporting cellular turnover and structural reinforcement.
These processes collectively underpin endurance, load tolerance, and the capacity for functional recovery following stress or injury.
Clinical Integration
From an integrated clinical perspective, arterial function must be understood as a dynamic system combining real-time perfusion and collateral support. Pulses reflect the immediate adequacy of blood flow, while anastomotic networks provide a reserve mechanism that safeguards tissue perfusion under physiological and pathological conditions.
Movement capacity therefore depends on both sufficient arterial supply and continuity of flow. Impairment at either level compromises tissue survival, reduces mechanical efficiency, and limits recovery potential, emphasizing the central role of arterial circulation in musculoskeletal health and function.
CLINICAL RELEVANCE
Ischema Tissue Viability
Disruption of arterial supply compromises continuous delivery of oxygen and metabolic substrates, leading to tissue ischemia and cellular dysfunction. Skeletal muscle and bone are highly metabolically active and therefore particularly vulnerable to reduced perfusion.
Prolonged ischemia results in ATP depletion, loss of ion homeostasis, and cellular necrosis, ultimately manifesting as functional impairment. Clinically, this underlies conditions such as arterial occlusion due to thrombosis, embolism, or atherosclerosis, where reduced blood flow leads to muscle weakness, pain, and potential tissue loss.
Vascular Injury
Trauma to arterial structures – whether from fractures, dislocations, or penetrating injuries – can directly compromise regional blood supply. Certain anatomical regions exhibit critical vascular dependence, where disruption of a single arterial source leads to severe consequences.
A key example is the femoral head, where interruption of its blood supply may result in avascular necrosis (AVN). This highlights the essential role of arterial integrity in maintaining bone viability and structural stability.
Compartment Syndrome
Compartment syndrome represents a pathophysiological state in which increased intracompartmental pressure exceeds capillary perfusion pressure, restricting arterial inflow and venous outflow. The resulting ischemia rapidly leads to muscle and nerve damage, making this a surgical emergency.
Without timely decompression, irreversible tissue necrosis and long-term functional loss occur, emphasizing the critical balance between vascular supply and mechanical constraints.
Surgical Rehabilitation
Preservation and restoration of arterial supply are central to clinical practice. In orthopedic and reconstructive surgery, adequate perfusion is essential for fracture healing, graft survival, and tissue regeneration. In sports medicine and rehabilitation, re-establishing vascular flow supports recovery, adaptation, and return to function. Consequently, detailed knowledge of arterial anatomy is fundamental for clinicians, as arterial integrity directly determines healing capacity, functional outcomes, and long-term musculoskeletal health.