
Clinical Relevance
Clinical evaluation of the musculoskeletal system requires interpretation of movement as the integrated output of a multiscale neuromuscular–biomechanical system. Skeletal muscle function is governed by α-motor neuron activation, motor unit recruitment dynamics, and excitation–contraction coupling, which together regulate force generation at the sarcomere level.
This force is transmitted through hierarchical connective tissue networks to produce joint torque, while proprioceptive feedback mechanisms – mediated by muscle spindles, Golgi tendon organs, and joint receptors – continuously modulate motor output to maintain stability and precision. As a result, observable movement reflects the coordinated interaction between neural control, muscle mechanics, and joint biomechanics.
Clinically, dysfunction may originate at any level of this system, including impaired neural activation, altered force transmission, or disrupted biomechanical alignment. However, such deficits rarely present in isolation; instead, they manifest as integrated movement impairments characterized by altered kinematics, reduced force efficiency, and compensatory motor strategies.
Accurate clinical assessment therefore requires differentiation between primary dysfunction and secondary adaptations, with evaluation of force production, movement coordination, and load distribution across the system. This systems-based approach is essential for precise diagnosis and the restoration of efficient, stable, and functionally adaptive movement.
CLINICAL RELEVANCE
Impared Force Generation
AI-Generated Illustration-MyoAnatomy
Mechanism
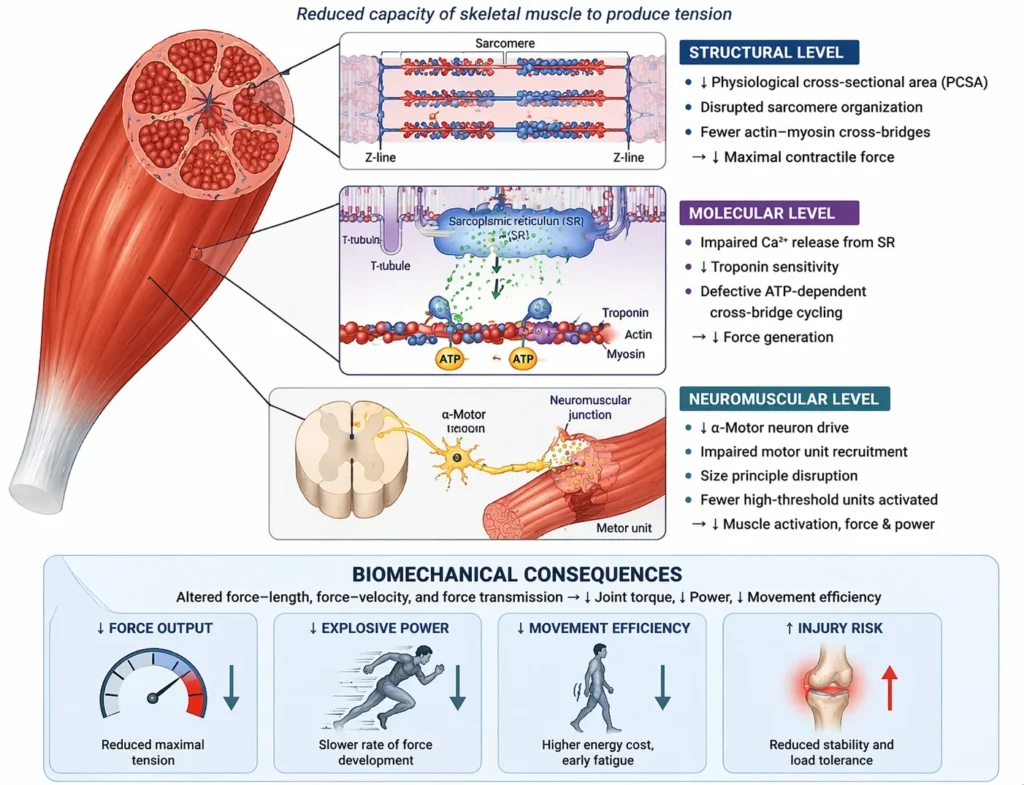
Impaired force generation arises from structural, neural, and metabolic alterations that reduce the capacity of skeletal muscle to produce tension. At the structural level, a reduction in physiological cross-sectional area (PCSA) and disruption of sarcomere organization decrease the number of functional actin–myosin cross-bridges available for force production, thereby lowering maximal contractile output.
At the molecular level, alterations in excitation–contraction coupling—including impaired Ca²⁺ release from the sarcoplasmic reticulum, reduced troponin sensitivity, or defective ATP-dependent cross-bridge cycling—further limit force generation.
At the neuromuscular level, decreased α-motor neuron drive and impaired motor unit recruitment (size principle disruption) reduce the effective activation of muscle fibers, particularly high-threshold units responsible for peak force and power.
Biomechanically, these changes alter the force–length relationship (suboptimal sarcomere overlap), impair the force–velocity relationship (reduced power output), and compromise efficient transmission of force through connective tissue networks (endomysium → perimysium → epimysium → tendon).
Collectively, these mechanisms result in diminished maximal tension, reduced rate of force development, and impaired functional performance across the range of motion.
Exam Question
Explain the multilevel mechanisms underlying impaired skeletal muscle force generation, including structural (PCSA and sarcomere integrity), molecular (excitation–contraction coupling), and neural (motor unit recruitment) factors, and discuss how these alterations affect force–length and force–velocity relationships.
Functional Consequence
Reduced force generation directly compromises joint torque production, limiting the ability to initiate and sustain effective movement. As a consequence, dynamic joint stabilization is impaired, leading to increased reliance on passive stabilizing structures such as ligaments, joint capsules, and articular surfaces.
This shift in load distribution increases mechanical stress on non-contractile tissues, predisposing to microtrauma, overuse injuries, and progressive structural degeneration. In addition, inefficient force production elevates the metabolic cost of movement, resulting in early onset of fatigue and reduced endurance capacity.
Altered neuromuscular coordination further disrupts movement efficiency, often leading to compensatory recruitment of adjacent muscle groups and abnormal movement patterns, which amplify biomechanical inefficiency and injury risk.
Exam Question
Describe the functional consequences of impaired muscle force generation on joint mechanics, stability, and load distribution, and explain how these changes contribute to fatigue, compensatory movement strategies, and increased injury risk.
Clinical Analysis
Clinically, impaired force generation manifests across a spectrum of conditions characterized by reduced muscle mass, altered neuromuscular activation, or intrinsic contractile dysfunction.
Tisuse atrophy results from reduced mechanical loading, leading to rapid decreases in muscle cross-sectional area and motor unit activation efficiency.
Sarcopenia reflects age-related declines in muscle mass, preferential loss of fast-twitch fibers, and impaired neuromuscular transmission, resulting in reduced strength and power.
Myopathies involve intrinsic defects in muscle fibers, including abnormalities in contractile proteins, mitochondrial function, or metabolic pathways, directly impairing force production at the cellular level.
Importantly, muscle weakness should be interpreted not merely as a deficit in strength, but as a failure of integrated force generation within a load-bearing system. This leads to impaired joint control, altered kinematics, and progressive mechanical overload of surrounding tissues.
Clinically, this manifests as joint instability (e.g., quadriceps weakness leading to knee instability), compensatory muscle overuse, and increased risk of degenerative joint disease due to chronic abnormal loading patterns.
Exam Question
Analyze the clinical presentation of impaired muscle force generation across conditions such as disuse atrophy, sarcopenia, and myopathies, and explain how deficits in force production lead to joint instability, compensatory muscle activity, and progressive degenerative changes.
Disrupted Neural Control
AI-Generated Illustration-MyoAnatomy
Mechanism
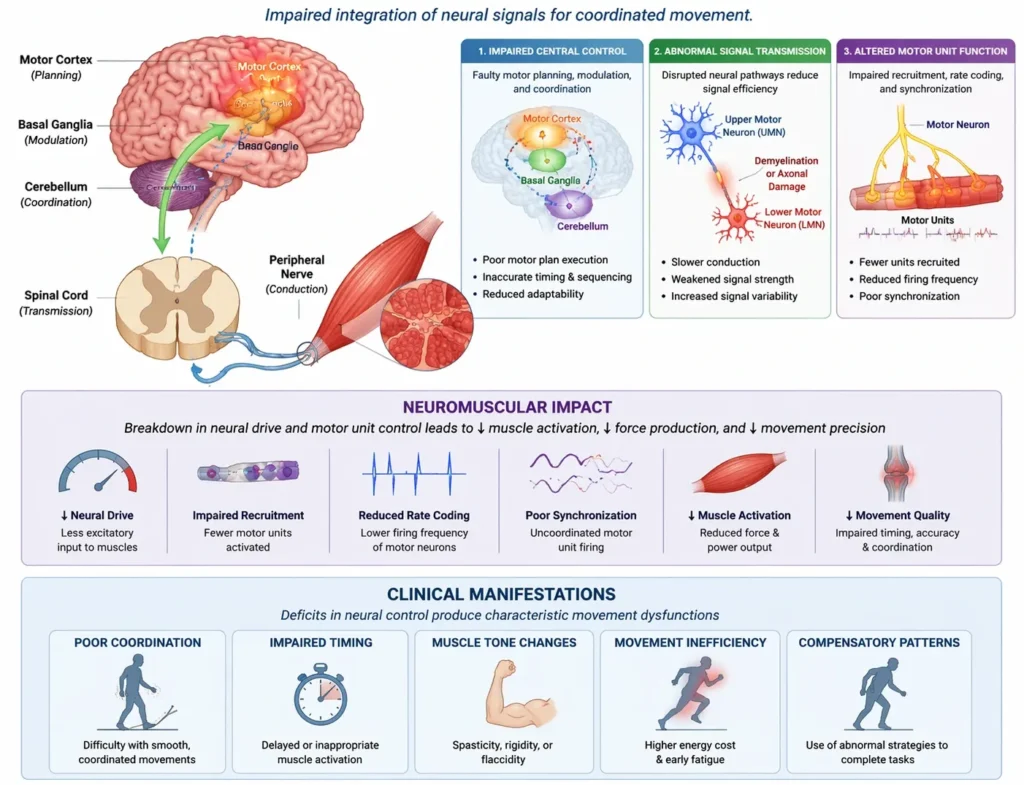
Efficient movement depends on the integration of central and peripheral neural systems, coordinating motor planning, execution, and real-time feedback. This process involves hierarchical control from the motor cortex, modulation by basal ganglia and cerebellum, and execution via spinal motor circuits and peripheral nerves.
At the motor unit level, force output is regulated through precise recruitment (size principle), rate coding (firing frequency), and synchronization of motor units. Concurrently, proprioceptive input from muscle spindles, Golgi tendon organs, and joint receptors continuously modulates motor output via reflex pathways and supraspinal feedback loops.
Disruption at any level of this system leads to impaired neural drive, characterized by reduced or inappropriate activation of muscle fibers. Temporal coordination is compromised, resulting in defective sequencing and timing of muscle contractions. Additionally, impaired sensorimotor integration reduces the accuracy of proprioceptive feedback, limiting the nervous system’s ability to adapt movement to changing mechanical demands.
These alterations degrade the capacity of the neuromuscular system to generate smooth, efficient, and task-specific motor output, fundamentally impairing movement quality rather than solely force magnitude.
Exam Question
Explain how disruption of central and peripheral neural control affects motor unit recruitment, rate coding, and sensorimotor integration, and analyze how these changes impair movement coordination and adaptability.
Functional Consequence
Disrupted neural control primarily affects the quality, coordination, and adaptability of movement. Impaired temporal sequencing leads to deficits in coordinated multi-joint actions, particularly during complex or rapid tasks requiring precise timing.
Alterations in muscle tone – manifesting as spasticity (velocity-dependent hypertonia), rigidity (uniform resistance), or flaccidity (reduced tone) – disturb normal resistance to movement and compromise functional joint control. These changes reflect underlying imbalances in excitatory and inhibitory neural pathways.
Loss of fine motor control and joint position sense results from impaired proprioceptive processing, reducing movement precision and accuracy. Consequently, the ability to adjust motor output in response to changing environmental or mechanical conditions is diminished.
Overall, movement becomes inefficient, poorly graded, and less adaptable, increasing reliance on compensatory strategies and predisposing to functional limitation and injury.
Exam Question
Describe the functional consequences of disrupted neural control on movement coordination, muscle tone, and proprioception, and explain how these alterations impair adaptability and precision of motor output.
Clinical Analysis
Clinically, disrupted neural control presents with distinct patterns depending on the level of the lesion.
Upper motor neuron (UMN) lesions result in spasticity, hyperreflexia, and stereotyped movement patterns due to loss of inhibitory supraspinal control. This leads to exaggerated reflex activity and reduced selective motor control.
Lower motor neuron (LMN) lesions cause deprevation, flaccid paralysis, fasciculations, and rapid muscle atrophy, reflecting direct loss of neural input to muscle fibers.
Neuromuscular junction disorders, such as myasthenic conditions, impair synaptic transmission, producing fatigable weakness characterized by preserved initial strength with progressive decline during repeated activity.
Importantly, neuromuscular dysfunction transforms movement from a quantitatively reduced output (weakness) into a qualitatively disorganized process. Impairments in timing, coordination, and motor control lead to abnormal synergy patterns, co-contraction of antagonistic muscles, and inefficient, rigid, or poorly graded movements.
Clinically, this manifests as impaired task execution, reduced movement efficiency, and increased energy expenditure, often accompanied by compensatory motor strategies and progressive functional decline.
Exam Question
Compare the clinical features of upper motor neuron, lower motor neuron, and neuromuscular junction disorders, and explain how each disrupts neural control to produce distinct patterns of movement dysfunction.
Impared Force Transmission
AI-Generated Illustration MyoAnatomy
Mechanism
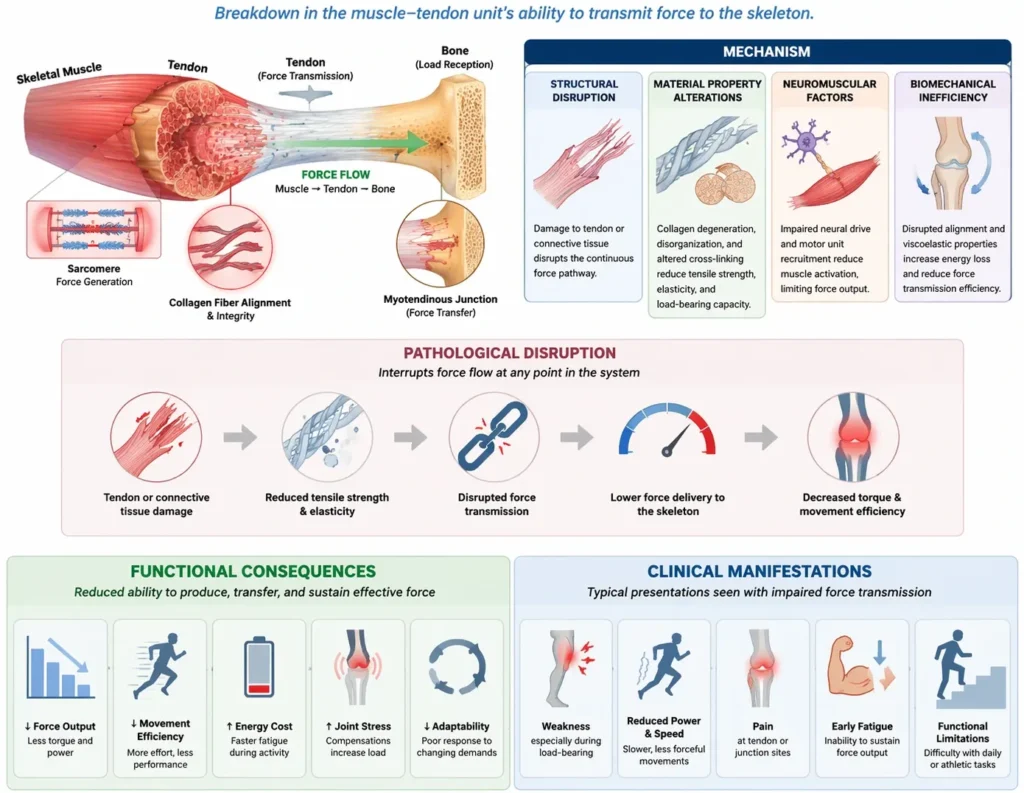
Force transmission from muscle to skeleton depends on the integrity of a continuous myotendinous and connective tissue network, including intramuscular connective tissues (endomysium, perimysium, epimysium) and tendons. This system converts sarcomere-generated force into joint movement through both longitudinal (fiber-to-tendon) and lateral (fiber-to-matrix) transmission pathways.
The efficiency of this process is determined not only by structural continuity but also by the viscoelastic properties of the extracellular collagen matrix, which enable optimal load transfer and elastic energy storage.
Pathological disruption occurs through:
Mechanical discontinuity → partial or complete rupture of tendon or connective tissue interrupts force transmission despite preserved contractile capacity
Material property alteration → collagen degeneration, disorganization, and altered cross-linking reduce tensile strength, elasticity, and load-bearing capacity
Matrix–fiber uncoupling → impaired lateral force transmission due to disruption of cytoskeletal – extracellular matrix connections (e.g., costameres
These alterations reduce the efficiency with which contractile force is transmitted, leading to a dissociation between muscle activation and effective movement output.
Exam Question
Explain the mechanisms of force transmission from muscle to skeleton, distinguishing between longitudinal and lateral pathways, and analyze how mechanical discontinuity and altered collagen properties impair effective force transfer.
Functional Consequence
Impaired force transmission results in a reduction of effective force delivery to the skeleton despite preserved or partially preserved muscle contractility. Consequently, joint torque production is diminished, and movement efficiency is reduced.
Loss of elastic energy storage and recoil within tendinous structures increases the metabolic cost of movement, particularly during cyclic activities such as gait and running.
Pain associated with connective tissue pathology further contributes to reflex inhibition of muscle activation, exacerbating functional deficits.
Biomechanically, impaired transmission alters moment arm efficiency and force–time characteristics, reducing the capacity for rapid force development and explosive movements. Additionally, disruption of elastic recoil mechanisms compromises activities dependent on stretch – shortening cycles.
Overall, movement becomes less coordinated, less efficient, and mechanically compromised across multiple joints.
Exam Question
Discuss the functional consequences of impaired force transmission on joint torque, energy efficiency, and elastic recoil, and explain how these changes affect dynamic movements such as gait and explosive actions.
Clinical Analysis
Clinically, impaired force transmission is most commonly associated with disorders of the muscle–tendon unit.
Tendinopathy is characterized by collagen disorganization, increased ground substance, and reduced tensile strength, leading to decreased load-bearing capacity and inefficient force transfer.
Partial or complete tendon rupture produces mechanical discontinuity, resulting in a loss of effective force transmission despite intact muscle contraction, often presenting as profound functional weakness.
Chronic overuse injuries lead to cumulative microtrauma and failed healing responses, further degrading structural integrity and mechanical performance.
Critically, impaired force transmission represents a failure of the muscle–tendon unit as a continuous mechanical system. In this context, muscle strength alone does not predict functional performance, as force generated at the sarcomere level cannot be effectively translated into movement.
Clinically, this manifests as:
Weakness disproportionate to measured muscle strength
Pain-associated limitation of movement
Reduced mechanical efficiency and altered movement patterns
These features contribute to compensatory strategies, increased injury risk, and progressive dysfunction.
Exam Question
Evaluate the clinical significance of impaired force transmission in conditions such as tendinopathy and tendon rupture, and explain why functional weakness may occur despite preserved muscle contractile capacity.
Altered Joint Mechanics
AI-Generated Illustration-MyoAnatomy
Mechanism
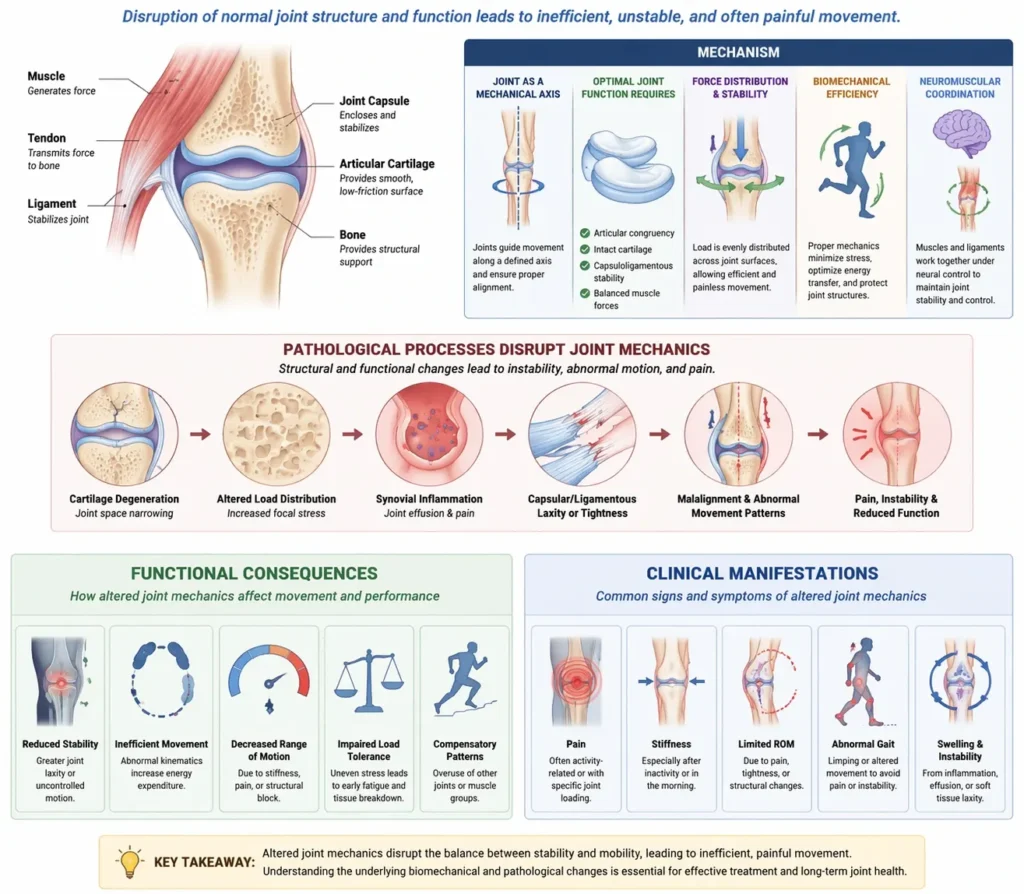
Joints define the mechanical axis of rotation and serve as the interface through which muscle-generated forces are translated into controlled movement. Optimal joint function depends on precise articular congruency, intact cartilage surfaces, balanced capsuloligamentous constraints, and full, pain-free range of motion.
At a biomechanical level, joint stability and efficiency rely on uniform load distribution across articular surfaces and coordinated interaction between active (muscular) and passive (ligamentous, capsular) stabilizing systems.
Pathological processes disrupt this system through:
Loss of joint congruency → altered contact mechanics leading to uneven stress distribution and focal overload
Restricted or excessive range of motion → capsular stiffness, structural deformity, or pain-mediated guarding limiting normal kinematics
Altered load transmission → increased focal stress on cartilage, subchondral bone, and periarticular structures
These changes shift joint kinematics away from optimal patterns, impairing the efficient conversion of muscular force into controlled, coordinated movement and predisposing to progressive mechanical dysfunction.
Exam Question
Explain how alterations in joint congruency, range of motion, and load distribution disrupt normal joint mechanics, and analyze their effects on movement efficiency and tissue loading
Functional Consequence
Altered joint mechanics compromise both stability and movement efficiency. Arthrogenic muscle inhibition, driven by joint pathology and altered afferent input, reduces activation of stabilizing muscles, further destabilizing the joint.
Abnormal joint kinematics – such as altered tracking, axis deviation, and disrupted movement trajectories – lead to inefficient force application and increased mechanical stress on adjacent joints and soft tissues.
As a result, dynamic stability during load-bearing activities is reduced, and movement becomes less coordinated and more energy-demanding.
Compensatory adaptations emerge, including redistribution of forces to adjacent joints or synergistic muscle groups. While initially protective, these adaptations often lead to maladaptive movement patterns, reinforcing abnormal loading conditions.
Over time, this results in progressive biomechanical imbalance, increasing the risk of secondary injury and degenerative changes across the kinetic chain.
Exam Question
Discuss the functional consequences of altered joint mechanics, including arthrogenic muscle inhibition, abnormal kinematics, and compensatory adaptations, and explain how these contribute to progressive biomechanical dysfunction
Clinical Analysis
Clinically, altered joint mechanics are a central feature of both degenerative and inflammatory joint disorders.
In osteoarthritis, progressive cartilage degeneration, joint space narrowing, and subchondral bone remodeling disrupt load distribution, leading to stiffness, reduced range of motion, and mechanical pain.
Inflammatory arthritis involves synovial inflammation, joint effusion, and capsular distension, resulting in pain, instability, and impaired function.
Structural deformities – such as malalignment or post-traumatic changes – alter joint axes and force vectors, producing chronic mechanical overload and abnormal stress distribution.
Crucially, joint pathology fundamentally alters the mechanical environment of movement, transforming efficient force transmission into a compensatory and energetically inefficient process.
Clinically, this manifests as:
Persistent pain accompanied by secondary muscular dysfunction
Asymmetric and inefficient movement patterns
Progressive joint degeneration driven by abnormal load distribution
Exam Question
Analyze the clinical impact of altered joint mechanics in conditions such as osteoarthritis, inflammatory arthritis, and structural deformities, and explain how these changes lead to pain, altered movement patterns, and progressive degeneration.
Impaired Sensiromotor
AI-Generated Illustration MyoAnatomy
Mechanism
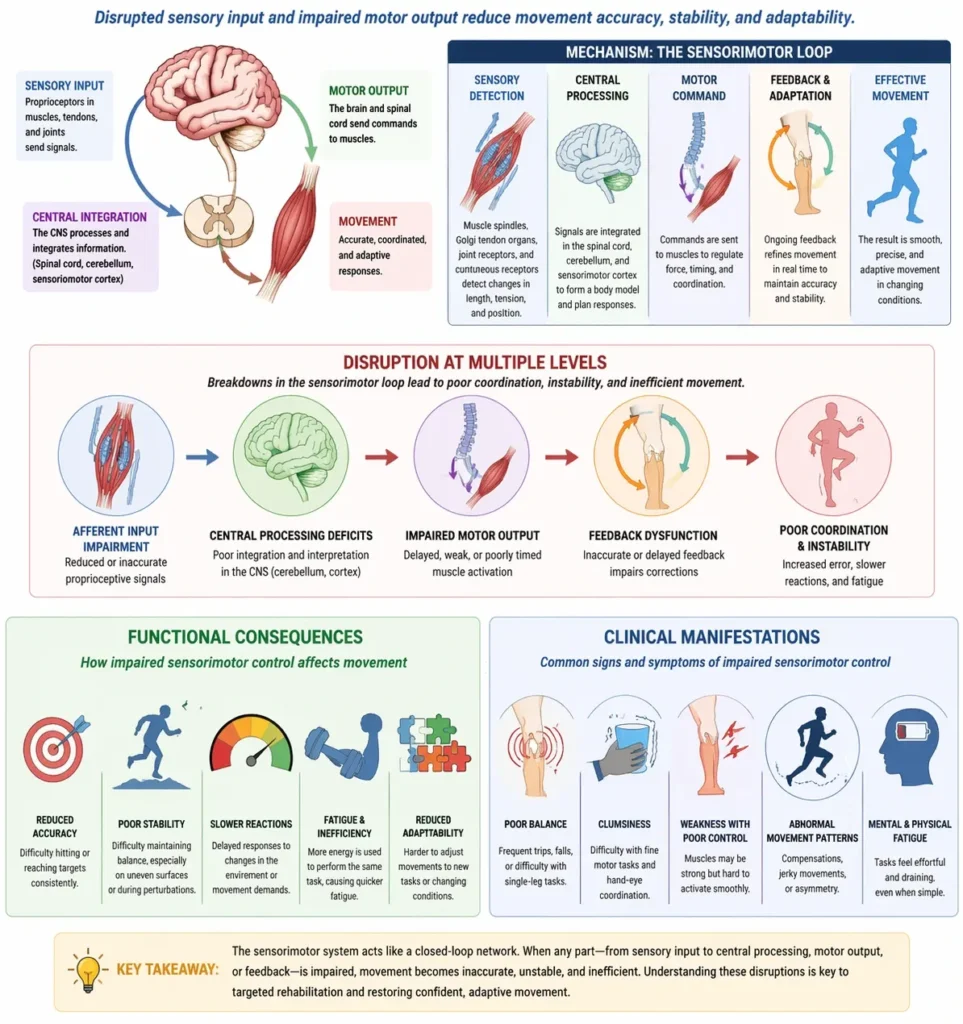
Efficient movement depends on continuous integration of afferent sensory input with efferent motor output within a closed-loop control system. Proprioceptive signals from muscle spindles (length and velocity), Golgi tendon organs (tension), joint receptors, and cutaneous mechanoreceptors provide real-time information regarding body position, movement, and load.
This sensory input is processed centrally within the spinal cord, cerebellum, and sensorimotor cortex, where it is integrated with motor commands to enable precise modulation of muscle activation, timing, and coordination.
Disruption of this system occurs at multiple levels:
Afferent input impairment → reduced or inaccurate proprioceptive signals from muscles, tendons, or joints
Central processing deficits → impaired integration and interpretation of sensory information within cerebellar or cortical networks
Reflex pathway dysfunction → altered or delayed spinal reflex responses affecting rapid motor adjustments
These disturbances impair feedback-driven motor control, reducing the nervous system’s ability to detect errors and adapt movement in real time. As a result, movement becomes less accurate, less stable, and poorly coordinated despite preserved muscle strength.
Exam Question
Explain the role of proprioceptive afferent input, central integration, and reflex pathways in sensorimotor control, and analyze how disruption at each level impairs feedback-driven movement regulation.
Functional Consequence
Impaired sensorimotor integration primarily affects movement accuracy, stability, and adaptability. Loss of joint position sense (proprioception) and kinesthesia reduces the ability to perceive limb orientation and motion, leading to decreased movement precision.
Delayed or inappropriate motor responses result from impaired feedback processing, limiting the ability to rapidly adjust muscle activity in response to perturbations or changing mechanical demands.
Consequently, dynamic joint stability is compromised, particularly during unpredictable or high-demand tasks, increasing reliance on passive stabilizing structures.
These deficits significantly increase the risk of injury and re-injury, as the system fails to detect and correct deviations from optimal movement patterns.
Overall, movement becomes unstable, poorly controlled, and less adaptable to environmental challenges.
Exam Question
Describe the functional consequences of impaired sensorimotor integration on proprioception, motor response timing, and joint stability, and explain how these deficits increase
Clinical Analysis
Clinically, impaired sensorimotor integration is observed across a range of musculoskeletal and neurological conditions.
Post-ligamentous injuries (e.g., anterior cruciate ligament disruption) reduce mechanoreceptor input, leading to diminished joint proprioception and impaired neuromuscular control.
Peripheral neuropathies disrupt sensory feedback pathways, resulting in decreased afferent input and impaired coordination.
Central nervous system disorders, including cerebellar or cortical dysfunction, impair integration and processing of sensory information, leading to deficits in coordination, balance, and movement precision.
Critically, movement dysfunction in these conditions may arise not from muscle weakness or structural damage, but from failure of sensory feedback integration within the motor control system.
Clinically, this manifests as:
A subjective “giving way” sensation despite adequate muscle strength
Impaired balance and coordination
Recurrent injuries due to inadequate neuromuscular control
Exam Question
Evaluate the clinical significance of impaired sensorimotor integration in conditions such as ligament injury, peripheral neuropathy, and central nervous system disorders, and explain how deficits in sensory feedback contribute to instability and recurrent injury.
CLINICAL EVALUATION
Range of Motion
AI-Generated Illustration -MyoAnatomy
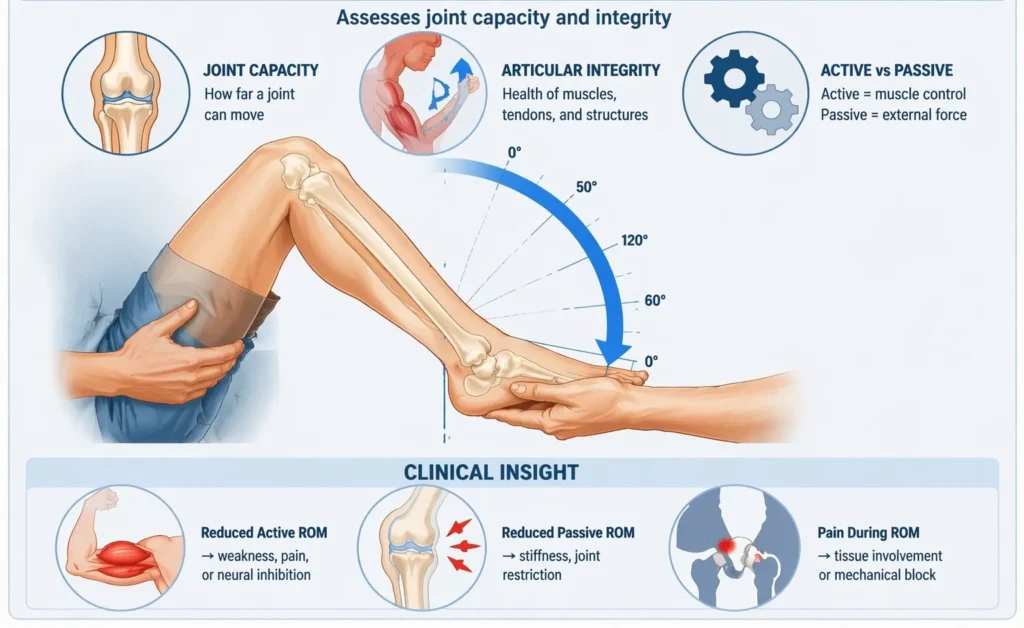
Range of Motion (ROM) assessment defines the mechanical capacity of a joint and evaluates the integrity of articular and periarticular structures. It differentiates between active ROM (reflecting neuromuscular function) and passive ROM (reflecting structural and mechanical constraints).
This distinction is critical for identifying the primary source of dysfunction:
Reduced active with preserved passive ROM → suggests muscular weakness, neural impairment, or pain inhibition
Reduced active and passive ROM → indicates structural restriction (capsular stiffness, ligamentous limitation, joint incongruity)
ROM analysis further identifies capsular patterns, characteristic limitations associated with specific joints, as well as non-capsular restrictions due to localized pathology.
Pain response during ROM provides insight into tissue involvement (contractile vs non-contractile), while abrupt mechanical limitation suggests structural block (e.g., loose body, osteophyte).
Clinically, ROM assessment establishes whether dysfunction is primarily mechanical (articular) or neuromuscular, guiding further evaluation.
Exam Question
Differentiate active and passive range of motion in clinical assessment, and explain how their comparison allows identification of muscular, neural, and structural causes of movement restriction.
Connective Tissue Organization
AI-Generated Illustration-MyoAnatomy
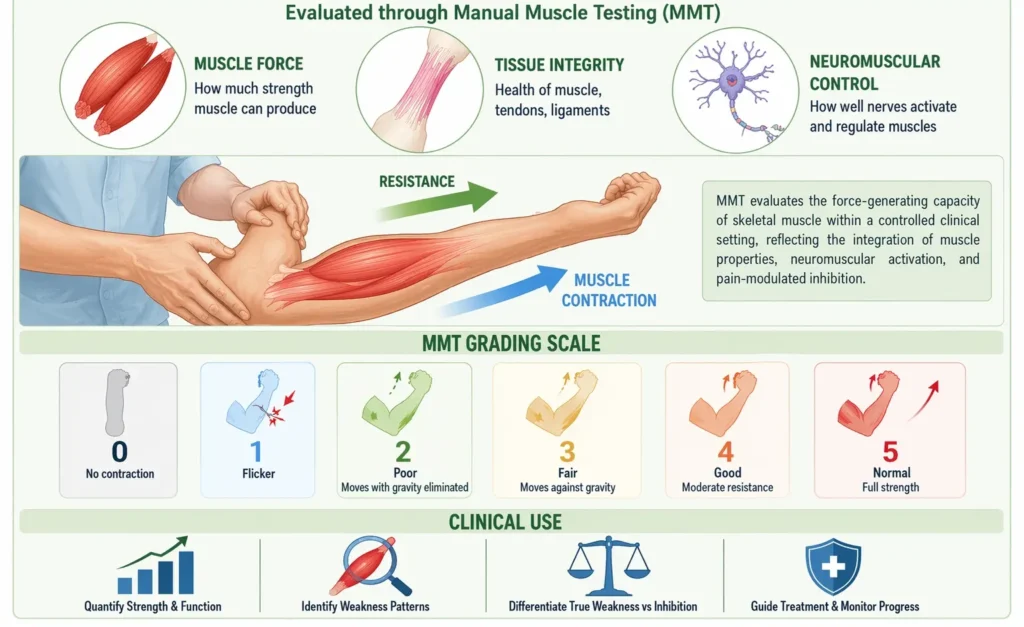
Manual Muscle Testing (MMT) evaluates the force-generating capacity of skeletal muscle within a controlled clinical setting. It reflects the integration of muscle contractile properties, neuromuscular activation, and pain-modulated inhibition.
MMT enables:
Quantification of muscle strength and functional integrity
Identification of weakness patterns across muscle groups
Differentiation between true muscular weakness and inhibition due to pain or neural dysfunction
At a mechanistic level, reduced strength may arise from decreased motor unit recruitment, impaired excitation–contraction coupling, or structural muscle changes (atrophy, fiber damage).
Patterns of weakness are clinically significant:
Myotomal distribution → suggests neural involvement
Global or symmetrical weakness → suggests systemic or myopathic process
Selective weakness with pain → suggests protective inhibition
Thus, MMT provides both functional and diagnostic insight, linking force production to neural and structural integrity.
Exam Question
Explain the principles of manual muscle testing and analyze how patterns of weakness can be used to differentiate between muscular, neurological, and pain-mediated causes of reduced strength.
Gait Analysis
AI-Generated Illustration-MyoAnatomy
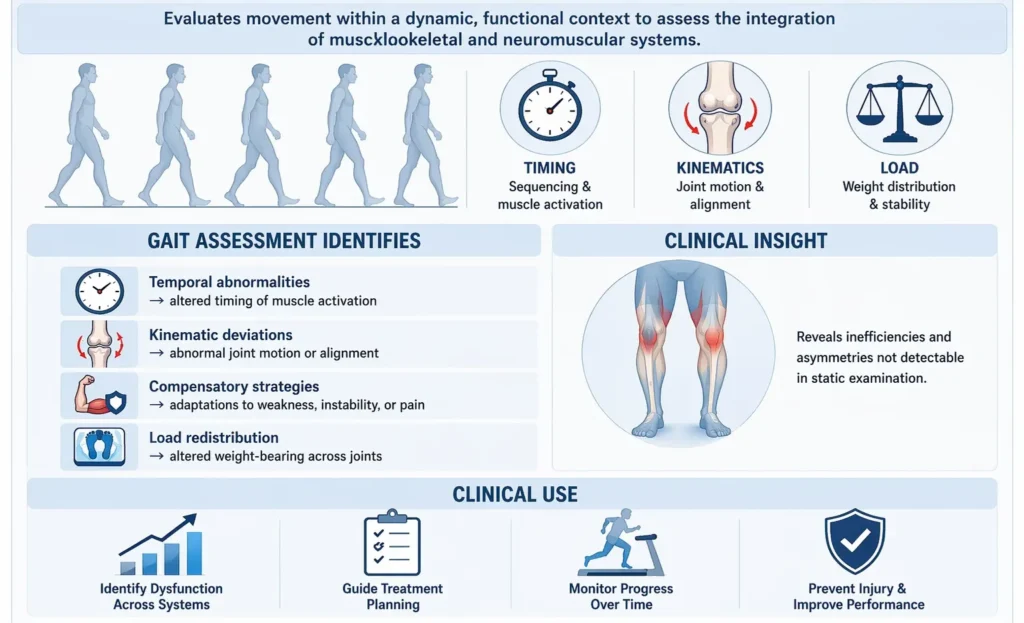
Gait analysis evaluates movement within a dynamic, functional context, reflecting the integrated performance of musculoskeletal and neuromuscular systems. Unlike isolated tests, it reveals system-level coordination, timing, and load distribution.
Normal gait requires precise sequencing of muscle activation, coordinated joint kinematics, and efficient energy transfer through the kinetic chain.
Gait assessment identifies:
Temporal abnormalities → altered timing and sequencing of muscle activation
Kinematic deviations → abnormal joint motion or alignment
Compensatory strategies → daptations to weakness, instability, or pain
Load redistribution → altered weight-bearing patterns across joints
These findings reveal inefficiencies and asymmetries not detectable in static examination.
Clinically, gait analysis exposes underlying dysfunction across multiple systems, including force generation, neural control, and joint mechanics, providing a comprehensive view of movement pathology.
Exam Question
Discuss the role of gait analysis in clinical assessment and explain how abnormalities in timing, coordination, and load distribution reveal underlying neuromuscular and biomechanical dysfunction.
Neurological Assessment
AI-Generated Illustration MyoAnatomy
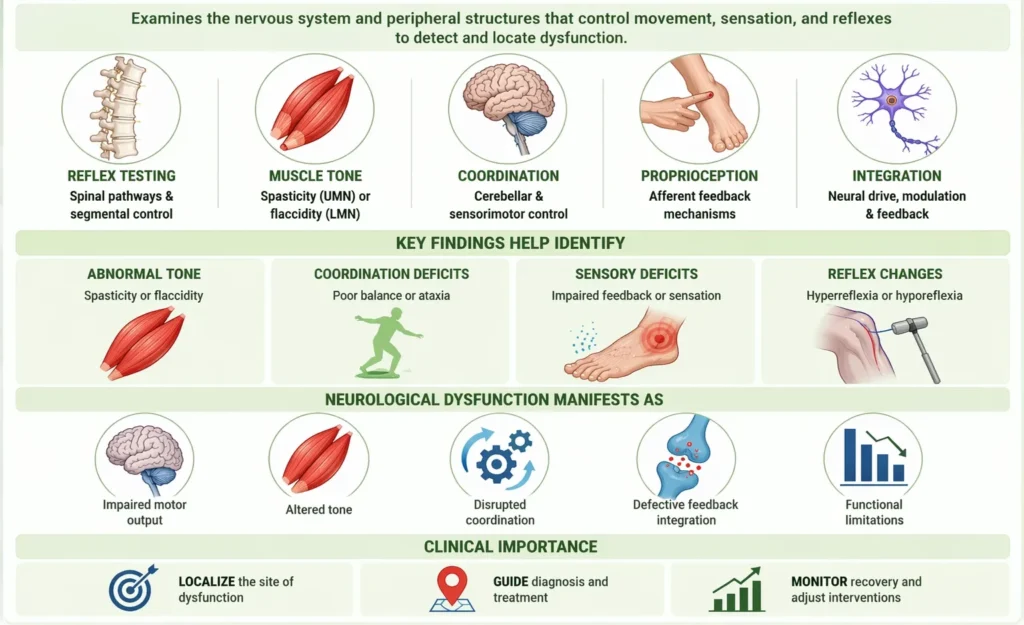
Neurological examination evaluates the integrity of central and peripheral systems responsible for motor control, sensory feedback, and reflex regulation.
Key components include:
Reflex testing → assesses integrity of spinal pathways and segmental control
Muscle tone evaluation → identifies abnormalities such as spasticity (UMN) or flaccidity (LMN)
Coordination testing → evaluates cerebellar and sensorimotor integration
Proprioceptive assessment → examines afferent feedback mechanisms
These elements collectively assess neural drive, modulation, and feedback control.
Neurological dysfunction manifests as impaired motor output, altered tone, disrupted coordination, and defective feedback integration.
Clinically, this assessment is essential for distinguishing neurological causes of dysfunction from primary musculoskeletal pathology, particularly when weakness, instability, or coordination deficits are present.
Exam Question
Describe the key components of neurological assessment in movement evaluation, and explain how reflexes, muscle tone, coordination, and proprioception help differentiate neurological from musculoskeletal dysfunction.