
Fibrous Joints
Fibrous joints are structurally stable articulations in which adjacent bones are united by dense collagen-rich connective tissue, without the presence of a synovial cavity. This architectural organization severely restricts or abolishes movement, thereby prioritizing mechanical stability, force transmission, and protection of critical anatomical structures.
In contrast to synovial joints, fibrous joints lack articular cartilage, a joint capsule, and synovial membrane. The intervening fibrous tissue – predominantly composed of type I collagen fibers – is arranged to resist tensile stress, enabling efficient load distribution across skeletal elements while maintaining structural integrity under mechanical demand.
Biomechanically, fibrous joints function as rigid or near-rigid units, optimized to withstand tensile and compressive forces without displacement. Their minimal compliance contributes to the preservation of spatial relationships between bones, particularly in regions requiring stability and protection, such as the cranial vault and dentoalveolar articulations.
Functionally and structurally, fibrous joints are classified into three principal subtypes – sutures, syndesmoses, and gomphoses – each reflecting variations in fiber organization, degree of permitted movement, and biomechanical role within the skeletal system.
SUTURES
AI -Generated Illustration-MyoAantomy
“Fibrous Joints” by OpenStax College, from Anatomy & Physiology, via Wikimedia Commons.
Licensed under CC BY 3.0
Definition
Fibrous joints are immobile or minimally mobile articulations in which adjacent bones are united by dense collagenous connective tissue without the presence of a synovial cavity. The interposed fibrous matrix – predominantly type I collagen – is organized to resist tensile forces, thereby stabilizing skeletal segments and preserving structural continuity.
These joints function as rigid mechanical linkages, optimized for force transmission and protection rather than movement. Their architecture minimizes displacement under load, ensuring maintenance of spatial relationships between bones, particularly in regions requiring high structural integrity such as the cranial vault.
Exam Question
In a biomechanical context, how does the collagen fiber orientation within fibrous joints determine their resistance to tensile forces and contribute to skeletal stability under load?
Structure
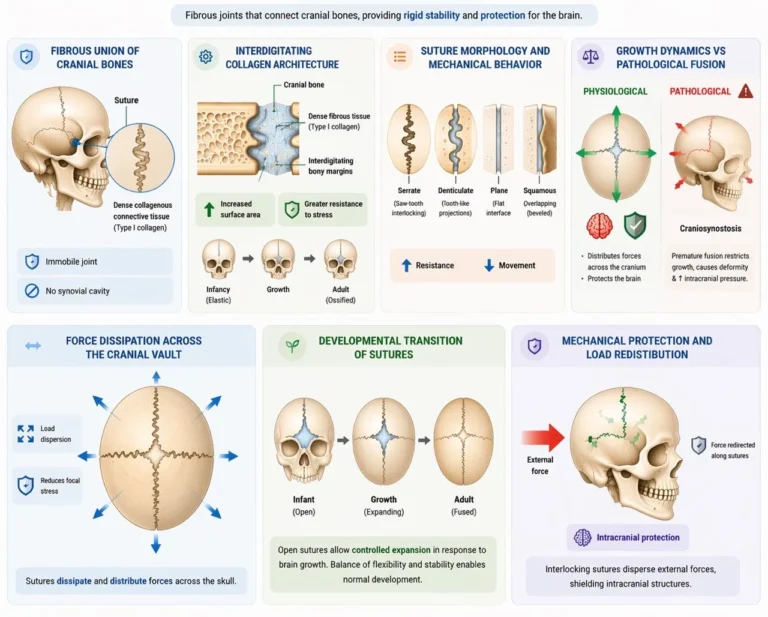
Sutures are specialized fibrous joints located exclusively between cranial bones, characterized by thin layers of dense connective tissue interposed between interdigitating bony margins. The complex interlocking geometry increases surface area and enhances resistance to mechanical stress.
During early development, sutures exhibit limited elasticity, permitting skull expansion in response to brain growth. With age, progressive ossification (synostosis) reduces compliance, transforming sutures into rigid unions that maximize protection of intracranial structures.
Biomechanically, sutures dissipate and distribute forces across the skull, preventing focal stress concentration and contributing to impact resistance.
Exam Question
Explain how the interdigitating morphology of sutures enhances force distribution and reduces stress concentration within the cranial vault?
Types
Sutures are classified according to the morphology of their articulating margins, which directly influences mechanical behavior:
Serrate sutures – saw-tooth interlocking; maximize resistance to tensile and shear forces (e.g., sagittal suture)
Denticulate sutures – deeper, tooth-like projections; provide enhanced mechanical interdigitation and stress resistance (e.g., lambdoid suture)
Plane sutures – relatively flat interfaces; allow minimal movement but maintain stability (e.g., internasal suture)
Squamous sutures – overlapping beveled edges; permit slight gliding while maintaining structural cohesion (e.g., temporoparietal suture)
The degree of interdigitation correlates with mechanical strength: greater complexity → higher resistance to deformation.
Exam Question
Correlate suture morphology with biomechanical function and explain why serrate sutures provide greater resistance to mechanical stress than plane sutures.
Functional & Clinical
Sutures function as rigid fibrous articulations that provide high mechanical stability through interdigitating bony margins and collagen-rich connective tissue, enabling efficient distribution of tensile and impact forces across the cranial vault. During early development, their limited elasticity permits controlled cranial expansion in response to brain growth while maintaining structural integrity. This balance between rigidity and minimal compliance allows sutures to act as force-dissipating interfaces, reducing focal stress and protecting intracranial structures.
Clinically, disruption of this balance leads to pathology. Premature fusion (craniosynostosis) restricts growth perpendicular to the affected suture, resulting in compensatory skull deformities and potential elevation of intracranial pressure. Conversely, suture diastasis reflects pathological separation due to trauma or increased intracranial pressure. Sutures also influence fracture propagation patterns, acting as zones of force redistribution. In infants, suture and fontanelle patency serves as an important indicator of neurological and hydration status.
Exam Question
How does the biomechanical architecture of cranial sutures simultaneously permit controlled cranial growth and ensure mechanical stability, and how do pathological alterations in this system manifest clinically?
SYNDESMOSIS
AI-Generated Illustration MyoAantomy
Definition
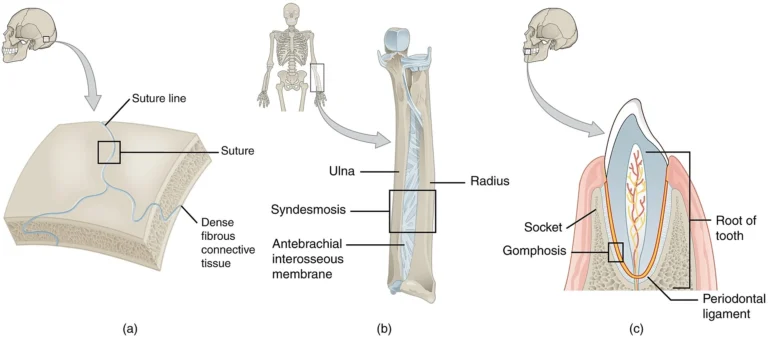
A syndesmosis is a fibrous joint in which adjacent bones are connected by elongated bundles of dense collagenous connective tissue, typically organized as ligaments or interosseous membranes. Unlike sutures, syndesmoses permit limited, controlled movement, the extent of which depends on fiber length, orientation, and elasticity.
From a biomechanical perspective, syndesmoses function as dynamic stabilizers, allowing slight displacement while maintaining alignment under tensile and rotational forces. Their structural organization enables force transmission between parallel bones, optimizing load distribution without compromising joint integrity.
Exam Question
Explain how the structural organization of a syndesmosis determines its capacity for controlled mobility while maintaining mechanical stability?
Components
The fibrous components of a syndesmosis are organized into:
Ligaments – discrete, collagen-rich bands that resist tensile and rotational forces
Interosseous membranes – broad, sheet-like structures connecting parallel long bones
Collagen fibers are highly oriented along lines of mechanical stress, providing resistance to traction and shear while permitting minimal deformation. This arrangement allows syndesmoses to function as load-sharing interfaces, redistributing forces across adjacent skeletal elements during movement.
Exam Question
Compare the biomechanical roles of ligaments and interosseous membranes within a syndesmosis, emphasizing their contribution to load transmission and stability.
Types
Key examples of syndesmoses include:
Distal tibiofibular syndesmosis – stabilizes the ankle mortise and maintains congruency during weight-bearing; reinforced by anterior/posterior tibiofibular ligaments and the interosseous ligament
Interosseous membrane of the forearm (radius–ulna) – distributes axial loads from the radius to the ulna and coordinates forearm rotational mechanics
Interosseous membrane of the leg (tibia–fibula) – provides longitudinal stability and facilitates force transmission during locomotion
These structures integrate stability with controlled compliance, ensuring efficient force propagation across limb segments.
Exam Question
Analyze how the distal tibiofibular syndesmosis contributes to ankle stability during weight-bearing and dynamic movement?
Functional & Clinical
Syndesmoses play critical biomechanical roles:
Stabilization of long bones during dynamic movement
Transmission and redistribution of mechanical loads
Maintenance of skeletal alignment under stress
Provision of attachment surfaces for muscles and fascia
Clinically, injury to a syndesmosis – most notably the distal tibiofibular syndesmosis – results in a high ankle sprain, typically caused by excessive external rotation or dorsiflexion. Disruption of this complex compromises joint stability, alters load distribution, and may lead to chronic instability or degenerative changes. Due to limited vascularity and high mechanical demand, healing is often prolonged and may require surgical stabilization.
Exam Question
Describe the biomechanical consequences of distal tibiofibular syndesmosis injury and explain why such injuries result in prolonged recovery compared to typical ligament sprains.
GOMPHOSIS
AI -generated illustration (MyoAantomy)
Definition
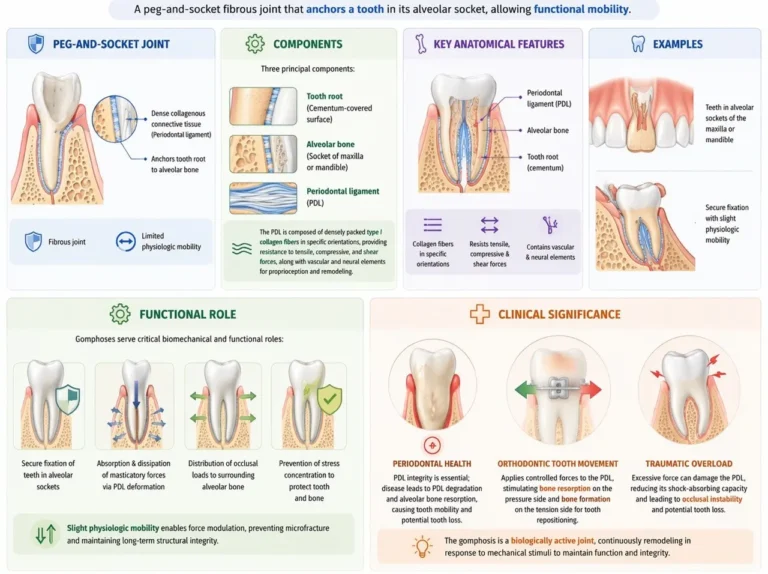
A gomphosis is a specialized fibrous joint characterized by a peg-and-socket articulation, in which the root of a tooth is anchored within the alveolar socket of the maxilla or mandible. This attachment is mediated by the periodontal ligament (PDL), a dense collagenous connective tissue that secures the tooth while permitting microscopic physiologic mobility.
Unlike other fibrous joints, gomphoses are uniquely adapted to withstand repetitive compressive and shear forces generated during mastication, functioning as a shock-absorbing anchorage system rather than a rigid fixation.
Exam Question
How does the structural organization of a gomphosis differ from other fibrous joints, and how does this specialization support its biomechanical function?
Components
The gomphosis consists of three principal components:
Tooth root (cementum-covered surface)
Alveolar bone (socket of maxilla or mandible)
Periodontal ligament (PDL)
The PDL is composed of densely packed type I collagen fibers arranged in specific orientations (e.g., oblique, horizontal, apical groups), allowing resistance to tensile, compressive, and shear forces. It also contains vascular and neural elements, enabling proprioception and adaptive remodeling.
This architecture transforms the gomphosis into a viscoelastic interface, capable of dissipating occlusal loads while maintaining firm anchorage.
Exam Question
Describe the role of the periodontal ligament in converting the gomphosis from a rigid attachment into a dynamic, load-adaptive structure.
Functional Role
Gomphoses serve critical biomechanical and functional roles: Secure fixation of teeth within alveolar sockets
Absorption and dissipation of masticatory forces through viscoelastic deformation of the PDL
Distribution of occlusal loads to surrounding alveolar bone
Prevention of stress concentration, protecting both tooth and bone
The slight physiologic mobility permitted by the PDL enables force modulation, preventing microfracture and maintaining long-term structural integrity under repetitive loading conditions.
Exam Question
Explain how the viscoelastic properties of the periodontal ligament contribute to force distribution and protection of the alveolar bone during mastication?
Clinical
Clinically, the integrity of the gomphosis is primarily dependent on the health of the periodontal ligament and surrounding alveolar bone.
Periodontal disease leads to inflammatory degradation of the PDL and alveolar bone resorption, resulting in tooth mobility and eventual tooth loss
Orthodontic tooth movement exploits the adaptive capacity of the PDL, where controlled mechanical forces induce bone resorption on the pressure side and bone formation on the tension side, enabling repositioning of teeth
Traumatic overload may disrupt the PDL, impairing its shock-absorbing capacity and leading to occlusal instability
Thus, the gomphosis represents a biologically active joint, capable of continuous remodeling in response to mechanical stimuli.
Exam Question
Explain the biological mechanisms underlying orthodontic tooth movement and relate them to the structural properties of the gomphosis.
FUNCTIONAL ROLE
Structural Stability
Fibrous joints provide maximal mechanical stability by firmly binding adjacent bones through dense collagenous connective tissue.
This rigidity is essential for maintaining precise anatomical alignment and preventing displacement under physiological and pathological loads, particularly in regions where movement would compromise structural integrity (e.g., cranial sutures).
Organs Protection
Fibrous articulations contribute directly to the formation of protective osseous compartments, particularly within the axial skeleton.
Cranial sutures interlock to create a continuous, mechanically integrated structure, enabling the skull to function as a unified load-bearing unit. External forces are thereby distributed across the entire cranial vault, reducing focal stress and protecting underlying neural tissue from mechanical injury.
This structural integration transforms individual bones into a functional protective system rather than isolated elements.
Force Transmission
Syndesmoses and interosseous membranes act as dynamic force-transmitting interfaces, facilitating the redistribution of mechanical loads between adjacent bones during movement.
Their collagen fibers are oriented along principal stress lines, enabling efficient load sharing and reduction of peak stress on individual skeletal elements. This enhances biomechanical efficiency, particularly during locomotion and weight-bearing activities, by coordinating force propagation across limb segments.
Thus, fibrous joints contribute not only to stability but also to integrated kinetic chain function.
Adaptive Anchoring
Fibrous joints provide secure yet adaptable anchorage, balancing fixation with controlled micro-mobility where required.
The gomphosis exemplifies this principle: the periodontal ligament introduces a viscoelastic interface that permits slight displacement under load. This micro-mobility enables absorption and dissipation of masticatory forces, preventing stress concentration while preserving positional stability of the tooth.
Such adaptive behavior reflects a key principle of fibrous joints – structural rigidity modulated by localized compliance to optimize both durability and function.
CLINICAL RELEVANCE
Cranial Fusion
Premature fusion of cranial sutures (craniosynostosis) disrupts the normal pattern of skull growth, which physiologically occurs perpendicular to suture lines. Early ossification eliminates this growth potential, resulting in compensatory expansion at remaining patent sutures and characteristic cranial deformities.
Biomechanically, loss of suture compliance reduces the skull’s ability to distribute mechanical forces, potentially contributing to elevated intracranial pressure and impaired neurodevelopment. This condition underscores the critical balance between structural stability and growth adaptability in fibrous joints.
Syndesmotic Instability
Injury to syndesmoses – most notably the distal tibiofibular syndesmosis – results in disruption of interosseous ligamentous tension and loss of joint congruency. This impairs the ability of the joint to effectively transmit and redistribute mechanical loads across the limb.
Biomechanically, instability leads to abnormal stress concentration, altered joint kinematics, and inefficient force propagation. Clinically, this manifests as persistent instability, impaired gait mechanics, and prolonged recovery, often exceeding that of typical ligamentous injuries due to the syndesmosis’ role in load-bearing integration.
Anchorage Loss
Degeneration of the periodontal ligament in the gomphosis compromises its function as a viscoelastic anchoring system, leading to progressive loss of tooth stability. As collagen fibers degrade and alveolar bone resorbs, the system loses its capacity for controlled load dissipation.
This results in tooth mobility, impaired mastication, and eventual tooth loss, reflecting failure of the delicate balance between rigidity and micro-mobility. The condition highlights the essential role of the periodontal ligament in maintaining functional anchorage under repetitive mechanical loading.
Joint Failure
Disruption of fibrous joints compromises their role in force transmission, structural stabilization, and load distribution, leading to abnormal biomechanical patterns across the musculoskeletal system.
Even minor alterations in these typically “immobile” joints can produce significant functional deficits, as forces are no longer efficiently dissipated. This results in stress redistribution to adjacent structures, compensatory movement patterns, and increased susceptibility to secondary injury.
Thus, fibrous joint failure illustrates that stability-based systems are integral to overall biomechanical efficiency, not merely passive structural elements.