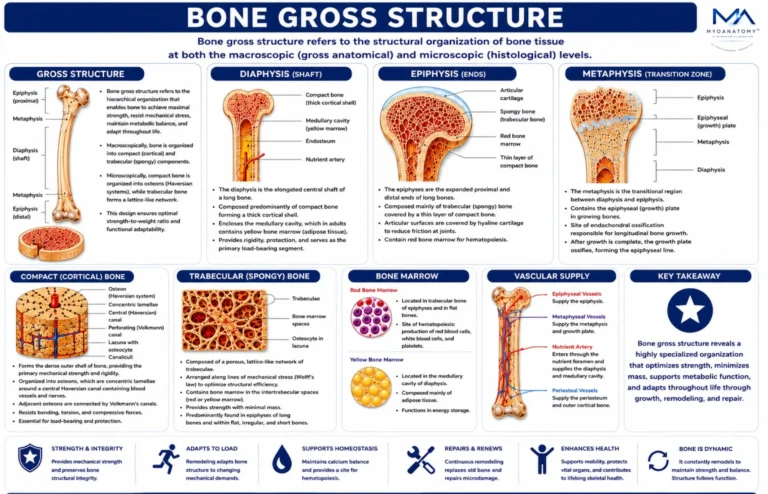
Trabecular (spongy) bone consists of a porous, lattice-like network of trabeculae, arranged along lines of mechanical stress, optimizing structural efficiency.
This architecture enables bone to resist compressive forces while minimizing overall skeletal mass, contributing to a favorable strength-to-weight ratio.
The intertrabecular spaces contain bone marrow:
Red marrow → hematopoiesis
Yellow marrow → fat storage(adipose tissue)
Trabecular bone is predominantly found in regions subjected to multidirectional loading, such as the epiphyses of long bones, vertebrae, pelvis, and ribs, where it facilitates force distribution and shock absorption.