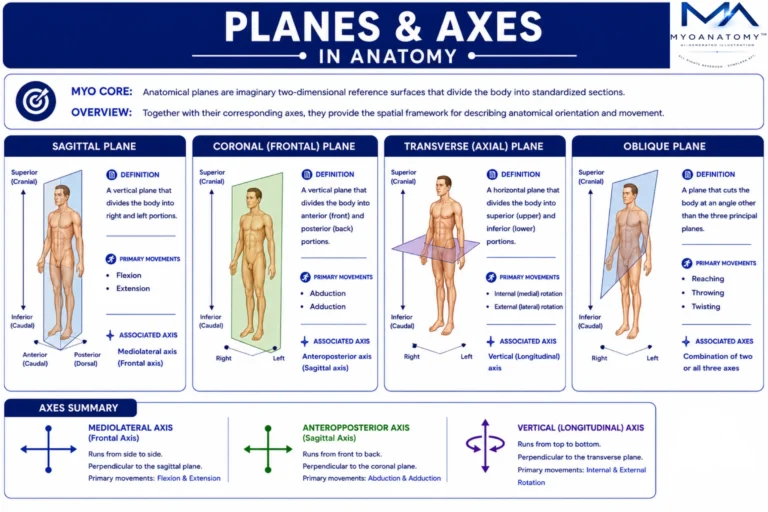
Although the three principal anatomical planes form the primary reference framework, many functional movements of the musculoskeletal system occur along oblique planes, which pass through the body at angles not aligned with sagittal, coronal, or transverse planes.
Oblique planes represent combinations of the principal planes and are characteristic of natural, coordinated human movement.
Example include reaching and throwing actions, twisting movements of the trunk and combined shoulder and hip motions.
In biomechanics and clinical movement analysis, recognition of oblique plane motion is essential for understanding integrated muscle function, joint coordination, and real life movement patterns.