
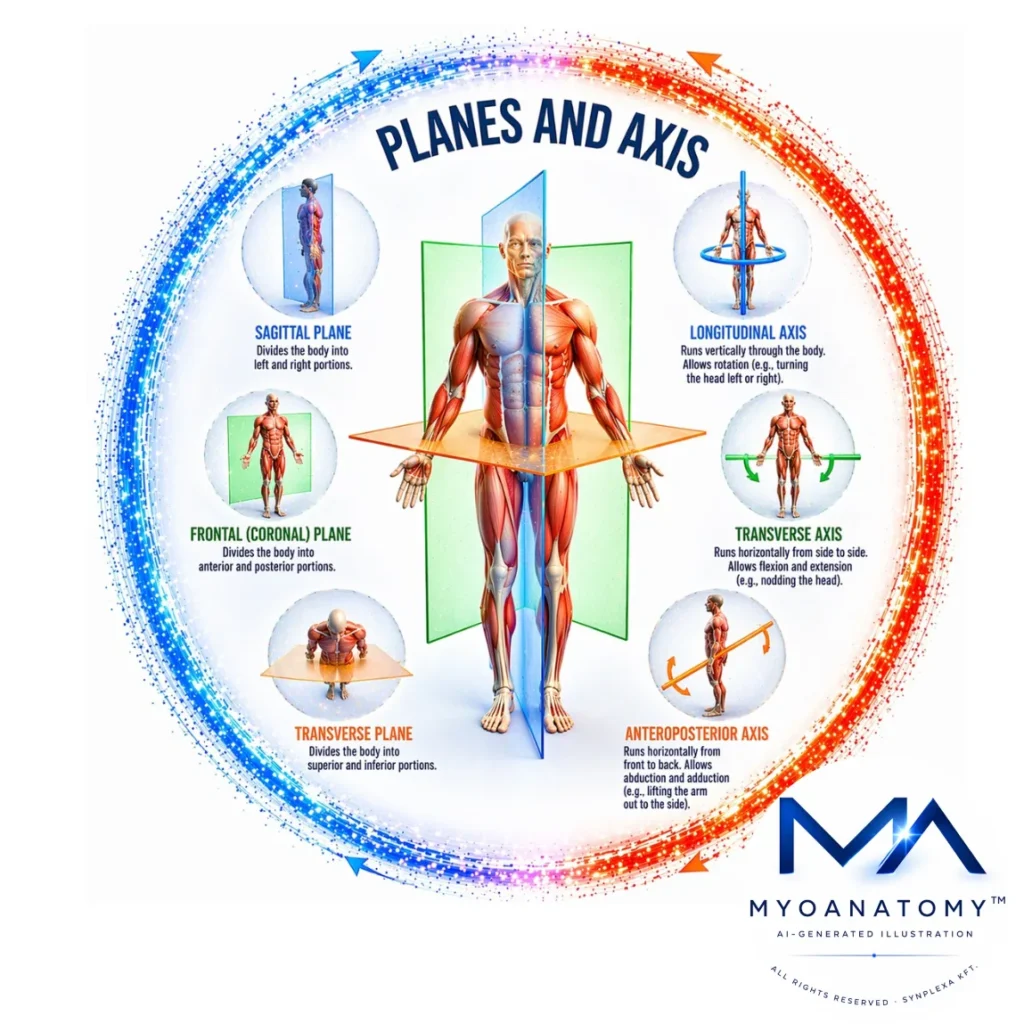
Planes & Axis
Anatomical planes are imaginary two-dimensional surfaces that divide body into sections and provide a standardized spatial framework for describing the orientation of structures and the direction of movements. These planes are defined relative to the anatomical position, ensuring that anatomical descriptions remain consistent regardless of the variations in posture during clinical examination, imaging, or movement analysis. In musculoskeletal anatomy and biomechanics, anatomical planes and their corresponding axis are essential for analysing joint motion, skeletal alignment, and muscular function. Each anatomical plane is associated with a perpendicular axis around which movement occurs.
ANATOMICAL PLANES
AI-Generated Illustration-MyoAnatomy
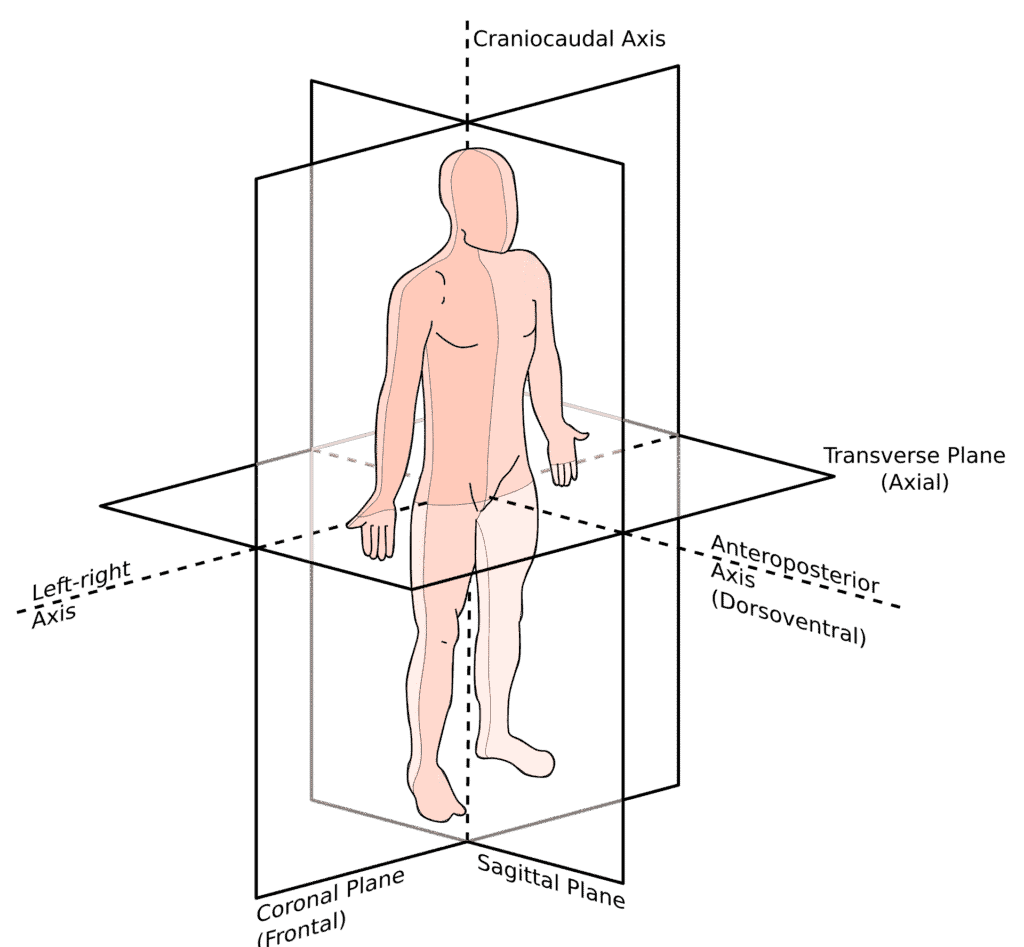
"Anatomical Planes" by Edoardo, via Wikimedia Commons. Licensed under CC BY-SA 3.0
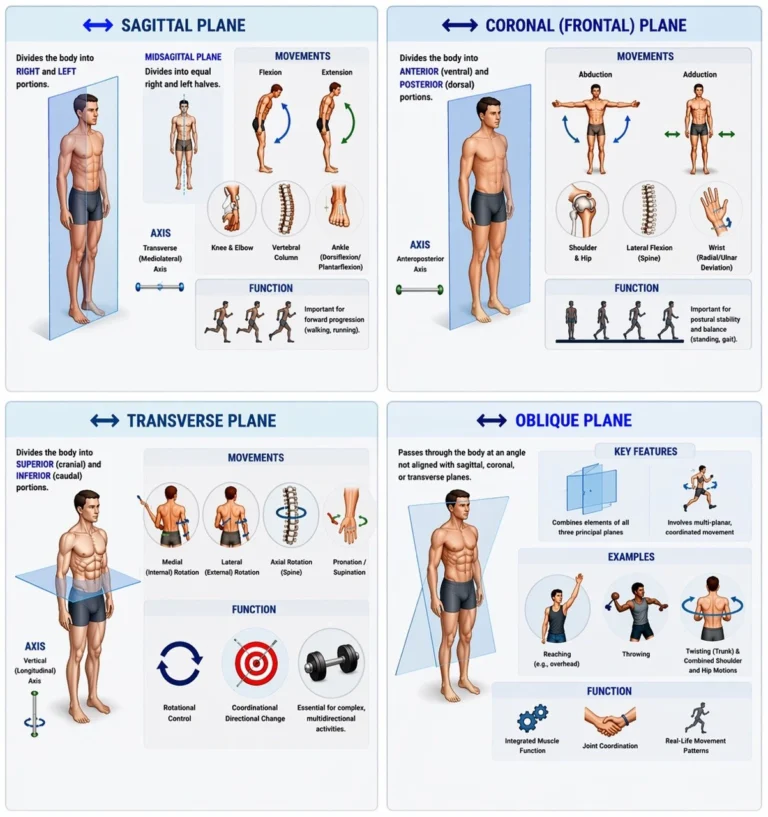
Sagital Plane
The sagittal plane is a vertical plane that divides the body into right and left portions. When it passes precisely through the midline it is termed the median (midsagittal) plane; planes parallel to it are referred to as parasagittal planes.
Movements occurring within the sagittal plane primarily involve flexion and extension, which alter the angle between adjacent skeletal segments. Typical examples include flexion and extension at the elbow, knee and hip joints; flexion and extension of the vertebral column; dorsiflexion and plantarflexion at the ankle joint.
Movements occur around a transverse ( mediolateral) axis.
Functionally, sagittal plane is particularly important for describing movement associated with forward progression such as walking and running.
Exam Question
In movement analysis, which anatomical plane defines flexion and extension of the elbow and knee, and along which axis do these movements occur?
Coronal ( Frontal) Plane
The coronal (frontal) plane, is a vertical plane that divides the body into anterior (ventral) and posterior (dorsal) portions.
Movements in this plane involve displacement toward or away from the body’s midline. The primary movements are: abduction and adduction of the shoulder and hip joints; lateral flexion of the vertebral column and radial and ulnar deviation at the wrist.
Movements occur around an anterior posterior axis.
Functionally movements in the coronal plane are important for maintaining postural stability and balance, particularly during standing and gait.
Exam Question
In functional movement, which anatomical plane defines abduction and adduction of the shoulder and hip, and around which axis do these movements occur?
Transverse Plane
The transverse plane (horizontal or axial) plane is a horizontal plane that divides the body into superior (cranial) and inferior (caudal) portions.
Movements in this plane involve rotational motion around a vertical (longitudinal) axis.
Primary movements include: medial (internal) rotation and lateral (external) rotation, axial rotation of the vertebral column, rotation of the head and neck, and pronation and supinationof the forearm
Functionally, the transverse plane is essential for describing movements involving rotational control, coordination, and directional change, particularly in activities. requiring complex, multidirectional motion.
Exam Question
In rotational movement, which anatomical plane defines medial and lateral rotation, and around which axis do these movements occur?
Oblique Plane
Although the three principal anatomical planes form the primary reference framework, many functional movements of the musculoskeletal system occur along oblique planes, which pass through the body at angles not aligned with sagittal, coronal, or transverse planes.
Oblique planes represent combinations of the principal planes and are characteristic of natural, coordinated human movement.
Example include reaching and throwing actions, twisting movements of the trunk and combined shoulder and hip motions.
In biomechanics and clinical movement analysis, recognition of oblique plane motion is essential for understanding integrated muscle function, joint coordination, and real life movement patterns.
Exam Question
In functional movement analysis, which anatomical plane describes motions not aligned with the principal planes and representing combined multi-planar activity?
FUNCTIONAL ROLE
Movement Planes
Anatomical planes provide a three-dimensional coordinate system for the human body, allowing movement to be described relative to standardized spatial orientations.
Each principal plane – sagittal, coronal (frontal), and transverse- is associated with a perpendicular axis of rotation and defines a primary category of movement.
Sagittal plane → flexion and extension
Coronal (frontal) plane → abduction and adduction
Transverse plane → rotational movements
This organization enables systematic classification and biomechanical analysis of movement across joints and body regions.
Multiplanar Motion
Although movements are often described within a single anatomical plane, most functional actions involve coordinated motion across multiple planes.
Anatomical planes provide a conceptual framework for decomposing complex movements into component vectors, enabling precise analysis of how joints and muscle groupscontribute to overall motion.
For example, gait involves sagittal plane motion (flexion and extension), coronal plane stabilization (pelvic control), and transverse plane rotation (rotational control of the trunk and limbs). Similarly, upper limb reaching integrates coordinated motion across all three planes.
Recognition of multiplanar motion is essential for understanding movement sequencing, interjoint coordination, and functional biomechanics in both normal and pathological states. Most real life human movements are inherently multiplanar requiring integrated neuromuscular control across all three anatomical planes.
Biomechanics Analysis
Anatomical planes serve as a standardized reference system in biomechanics, enabling consistent description of movement across individuals and clinical contexts.
This standardization allows:
comparison between normal and pathological movement patterns
quantitative motion analysis (e.g., gait analysis, joint kinematics)
reproducibility in research and clinical evaluation
They are essential for defining:
joint axes of rotation
muscle line of action
mechanical efficiency of movement
Muscle Mechanics
Muscle actions are interpreted relative to anatomical planes, with the orientation of a muscle determining both the plane of movement and the axis of rotation about which it acts.
For example:
muscles anterior to a joint → flexion (sagittal plane)
muscles lateral to a joint → abduction (coronal plane)
muscles crossing obliquely → rotational components (transverse plane)
This relationship is fundamental for understanding functional anatomy and movement mechanics.
The relationship between muscle line of action and joint axis determines the torque produced and thus the functional role of the muscles.
CLINICAL RELEVANCE
Clinical Assessmentt
Anatomical planes provide the fundamental framework for clinical evaluation of movement. During physical examination, joint motion is systematically assessed relative to specific planes to identify dysfunction patterns:
Plane-specific findings:
Sagittal plane restriction → impaired flexion/extension
Coronal (frontal) asymmetry → instability or muscle imbalance
Abnormal transverse rotation → neuromuscular or joint pathology
Clinical utility:
Localization of dysfunction
Assessment of range of motion (ROM)
Identification of compensatory movement patterns
Orthopaedetic Pathology
In orthopaedics, anatomical planes are essential for accurate description and classification of deformities and structural abnormalities.
Used to describe:
Fracture displacement
Joint deformities
Alignment abnormalities
High-yield examples:
Varus / Valgus deformities → coronal plane
Flexion contractures → sagittal plane
Rotational malignment → transverse plane
Imaging Analysis
Radiological imaging is fundamentally based on anatomical planes, which provide a standardized framework for spatial interpretation of internal structures.
Sectional interpretation:
Sagittal sections → profile view (anterior–posterior relationships)
Coronal sections → assessment of symmetry and lateral relationships
Axial (transverse) sections → cross-sectional anatomy
Clinical significance:
Accurate interpretation of CT, MRI, and ultrasound imaging requires precise understanding of anatomical planes to identify:
lesions
structural abnormalities
organ relationships
Clinical insights
Misinterpretation of imaging planes leads to diagnostic errors and incorrect localization of pathology.
Rehabilitation
In rehabilitation, anatomical planes provide a framework for targeted movement restoration and functional recovery strategies.
Core applications:
exercise prescription
movement retraining
functional recovery strategies
Therapeutic objectives:
restore movement within a specific plane
correct deficits in multiplanar coordination
improve stability across planes
High-yield examples:
Sagittal plane training → gait and mobility
Coronal plane control → balance and pelvic stability
Transverse plane control → rotational stability
ANATOMICAL AXIS
AI -Generated Illustration-MyoAantomy
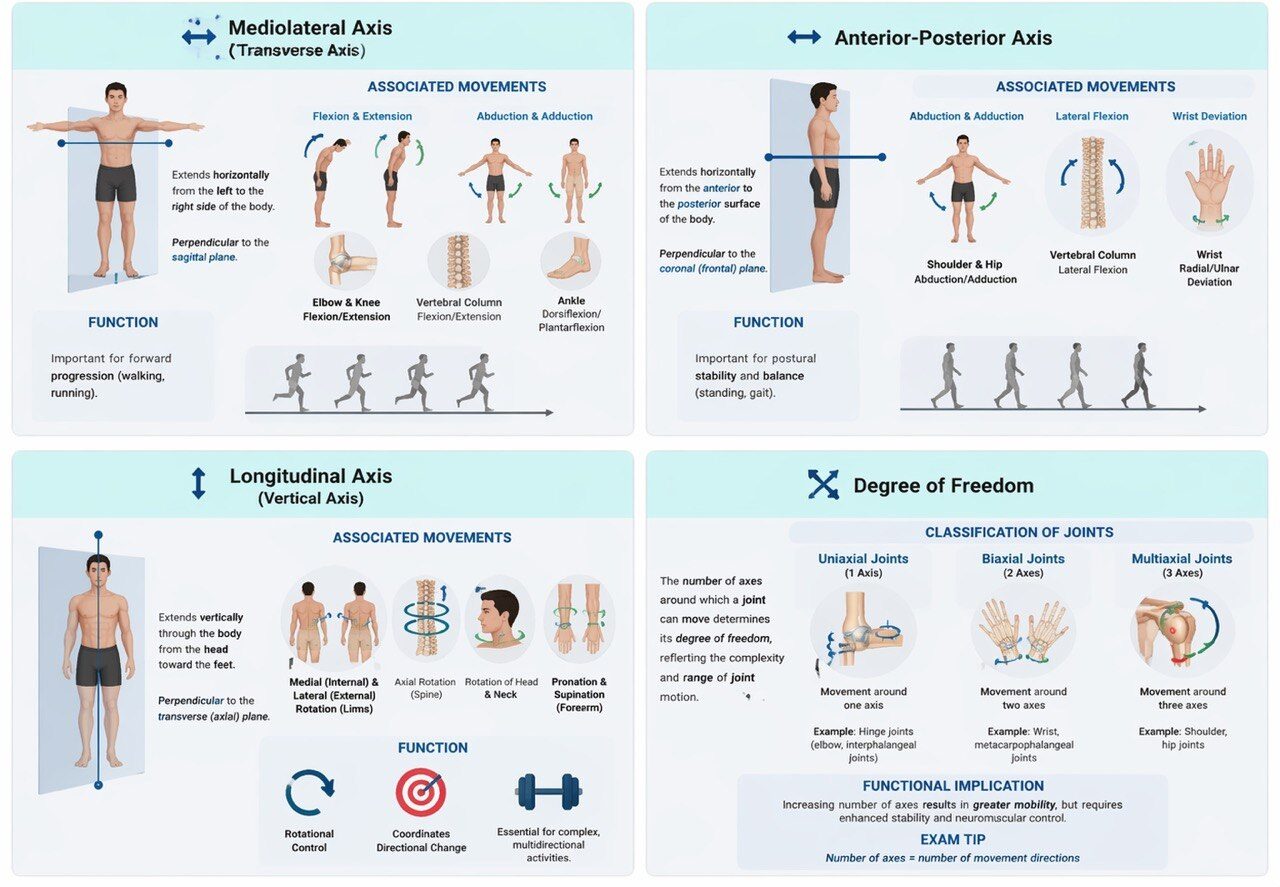
Mediolateral Axis
The mediolateral axis (transverse axis) extends horizontally from the left to the right side of the body.
It is perpendicular to the sagittal plane, and therefore all movements occurring within the sagittal plane rotate around this axis.
Associated movements:
flexion and extension
elbow flexion / extension
knee flexion / extension
hip flexion / extension
ankle dorsiflexion / plantarflexion
Exam Tip
Sagittal plane movements ALWAYS occur around the mediolateral (transverse) axis
Exam Question
How does the orientation of the mediolateral (transverse) axis, being perpendicular to the sagittal plane, explain its role in facilitating flexion and extension movements and determining the direction of angular motion across major joints?
Anterior-Posterior Axis
The anteroposterior axis extends horizontally from the anterior to the posterior surface of the body.
It is perpendicular to the coronal (frontal) plane, and movements within this plane rotate around this axis.
Associated movements:
abduction and adduction
shoulder and hip abduction/adduction
lateral flexion of the vertebral column
radial and ulnar deviation at the wrist
Exam Tip
Coronal plane movements ALWAYS occur around the anteroposterior axis
Exam Question
How does the anteroposterior axis, as the axis perpendicular to the coronal plane, govern abduction–adduction movements and influence lateral displacement and stability in the appendicular skeleton?
Longitudinal Axis
The longitudinal axis, also referred to as the vertical axis, runs vertically through the body from the head toward the feet.
It is perpendicular to the transverse (axial) plane, and movements occurring within this plane rotate around the longitudinal axis.
Associated movements:
medial (internal) rotation and lateral (external) rotation of the limbs
axial rotation of the vertebral column
rotation of the head and neck
pronation and supination of the forearm
Exam Tip
ALL rotational movements occur in the transverse plane around a longitudinal axis
Exam Question
How does the superior–inferior orientation of the longitudinal (vertical) axis, in relation to the transverse plane, determine the mechanics of rotational movements and coordination of axial and appendicular motion?
Degree of Freedom
The number of axes around which a joint can move determines its degree of freedom, reflecting the complexity and range of joint motion.
Classification of joints:
Uniaxial joints → movement around one axis→ example: hinge joints (elbow, interphalangeal joints)
Biaxial joints → movement around two axes→ example: wrist, metacarpophalangeal joints
Multiaxial joints → movement around three axes→ example: shoulder and hip joints
Functional implication:
Increasing number of axes results in greater mobility, but requires enhanced stability and neuromuscular control
Exam Tip
Number of axes = number of movement directions
Exam Question
How does the number of axes of movement in a joint determine its degree of freedom and influence the balance between mobility, structural stability, and neuromuscular control across different joint types?
FUNCTIONAL ROLE
Movement Organization
Anatomical axes provide the geometric framework through which movement is organized within the musculoskeletal system. By defining the lines of rotation, they establish precise spatial relationships between bones, joints, and muscle forces.
Movement is therefore not arbitrary, but structured and constrained by axes, which determine:
the direction of motion
the plane in which movement occurs
the interaction between anatomical structures
Functional principle:
This organization ensures that mechanical forces are transmitted in a controlled and predictable manner, allowing coordinated and efficient movement across the skeletal system.
Exam Tip: Axes define how movement occurs; planes define where movement occurs.
Force Transition
Anatomical axes enable the conversion of muscular contraction into coordinated joint movement. The line of action of a muscle relative to an axis determines the type and direction of motion produced.
Muscle contraction generates linear force, which is transformed into angular movement around an axis.
This transformation depends on: the position of the muscle relative to the axis; the orientation of the force vector; the structural characteristics of the joint
Functional principle:
Anatomical axes act as a reference system that links anatomical structure with biomechanical function, allowing precise and coordinated movement.
Exam Tip: Movement type is determined by the muscle’s position relative to the axis.
Joint Mechanics
Anatomical axes define the degrees of freedom (DOF) of a joint, determining the type and complexity of movement.
Uniaxial → one axis → single-plane motion → ↑ stability
Biaxial → two axes → combined motions
Multiaxial → three axes → multiplanar motion → ↑ mobility
Joint kinematics are governed by the interaction of articular geometry, ligaments, muscles, and neuromuscular control, producing coordinated and often coupled movements.
In vivo, motion occurs around a shifting instantaneous axis, not a fixed line, optimizing load distribution and mechanical efficiency.
Exam Tip
DOF = number of axes
More axes → more mobility, less stability
Real joint motion = dynamic (not fixed axis)
Dynamic coordination
In vivo joint motion occurs around a continuously shifting instantaneous axis of rotation, rather than a fixed anatomical axis, enabling adaptation to changing mechanical demands.
Movement is coordinated across multiple joints (kinetic chains) through integration of articular mechanics, muscle activity, and neuromuscular control.
This ensures:
efficient load distribution, preservation of joint congruency
optimization of stability and movement efficiency, whereas disruption leads to compensatory biomechanical patterns.
Exam Tip:
Dynamic coordination reflects multi-joint movement governed by a shifting instantaneous axis, requiring precise neuromuscular control to maintain efficiency and stability
CLINICAL RELEVANCE
Orthopedics
Deviations from physiological mechanical axes, such as varus or valgus alignment, result in asymmetric load distribution across articular surfaces, leading to focal cartilage overload, accelerated degeneration, and progressive joint pathology.
Chronic malalignment increases tensile stress on ligaments and alters joint kinematics, promoting instability and deformity progression.
Precise understanding of mechanical and anatomical axes is therefore essential for diagnosing deformities and guiding corrective interventions, including osteotomies and joint arthroplasty, where restoration of axis alignment is critical for long-term functional outcomes and implant longevity.
Physiotherapy
Anatomical axes provide the biomechanical framework for evaluating movement dysfunction, where disruption of the normal relationship between joint axes and muscular force vectors leads to inefficient or compensatory movement patterns.
Such alterations impair coordination, reduce mechanical efficiency, and increase energy expenditure.
Rehabilitation strategies aim to restore optimal alignment and neuromuscular control, re-establishing physiological movement patterns around appropriate axes to improve stability, function, and load distribution.
Sport Medicine
Biomechanical analysis relative to anatomical axes enables identification of movement inefficienciesand injury risk during dynamic activities.
Malalignment or poor control of joint axes, particularly during high-load tasks such as landing, cutting, or rotational movements, results in abnormal force transmission and increased stress on ligaments and tendons.
This contributes to injury mechanisms such as anterior cruciate ligament (ACL) rupture or chronic overuse syndromes, highlighting the importance of axis control in performance optimization and injury prevention.
Joint Instability
Alterations in the dynamic behavior of joint axes reflect underlying mechanical dysfunction, including ligamentous insufficiency, reduced joint congruency, or impaired neuromuscular control.
Such instability disrupts normal load distribution and joint tracking, leading to abnormal kinematics and progressive structural damage.
Accurate assessment of axis deviation and dynamic instability is therefore fundamental in clinical evaluation and in planning targeted interventions to restore stability and functional joint mechanics.