
Arterial Supply
Arterial supply is a high-pressure, hierarchically organized vascular system responsible for delivering oxygenated blood, metabolic substrates, and signaling molecules from the heart to peripheral tissues, forming the inflow component of systemic circulation. Blood is ejected from the left ventricle → aorta → elastic arteries → muscular arteries → arterioles → capillary beds, creating a branching network that enables both efficient bulk transport and precise regional regulation of perfusion.
Within the musculoskeletal system, arterial circulation is essential for maintaining metabolic activity, structural integrity, and functional performance of skeletal muscle, bone, joints, and connective tissues. At the cellular level, arterial perfusion sustains oxidative phosphorylation and ATP production, supports protein synthesis, collagen turnover, and bone remodeling, and enables tissue growth, repair, and adaptation to mechanical loading.
Blood flow is dynamically regulated through local metabolic mechanisms (hypoxia, ↑CO₂, ↓pH), endothelial signaling (nitric oxide-mediated vasodilation), and autonomic control, allowing rapid matching of perfusion to tissue demand—particularly in skeletal muscle, where energy requirements increase markedly during contraction. In addition to substrate delivery, arterial circulation contributes to thermoregulation, maintenance of biochemical homeostasis, and facilitation of downstream waste clearance, thereby functioning as a dynamic interface between cardiovascular output and musculoskeletal performance.
AI-generated illustration ( MyoAnatomy)
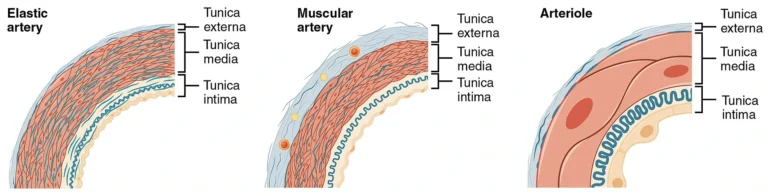
“Muscular and Elastic Artery, Arteriole ( Histological Schematic)” – OpenStax College, via Wikimedia Commons.
Licensed under CC BY 3.0
.
Description
The arterial system forms a hierarchically organized vascular network responsible for transporting oxygenated blood from the heart to peripheral tissues. Structurally and functionally, arteries are classified into several categories according to their diameter, wall composition, and physiological role in regulating blood flow. This organization allows the arterial circulation to efficiently distribute blood throughout the body while maintaining appropriate pressure and perfusion to tissues with varying metabolic demands.
The arterial wall itself typically consists of three concentric layers: the tunica intima, composed of endothelial cells lining the vessel lumen; the tunica media, containing smooth muscle and elastic fibers that regulate vessel diameter; and the tunica adventitia, a connective tissue layer providing structural support and anchoring the vessel to surrounding tissues. Variations in the thickness and composition of these layers account for the functional differences between the major categories of arteries.
Elastic Artery
Elastic arteries, also known as conducting arteries, represent the largest vessels of the arterial system and receive blood directly from the heart. Their walls contain a high concentration of elastic fibers within the tunica media, allowing these vessels to expand during ventricular systole and recoil during diastole.
This elastic recoil mechanism plays a crucial role in maintaining continuous blood flow and stabilizing arterial pressure between heartbeats. By dampening the pulsatile output of the heart, elastic arteries ensure smoother blood flow to distal regions of the circulation.
Major examples of elastic arteries include:
aorta
pulmonary trunk
common carotid arteries
subclavian arteries
These vessels serve primarily as major conduits distributing blood from the heart to large regional arterial branches, supplying the head, trunk, and limbs.
Muscular Artery
Muscular arteries, often referred to as distributing arteries, arise from elastic arteries and deliver blood to specific organs and anatomical regions. Their walls are characterized by a prominent tunica media composed predominantly of smooth muscle cells, which allows these vessels to actively regulate blood flow.
Through vasoconstriction and vasodilation, muscular arteries adjust their diameter in response to neural, hormonal, and local metabolic signals. This ability enables precise control of regional blood distribution, particularly during changes in physiological demand such as exercise or stress.
Examples of major muscular arteries include:
brachial artery supplying the upper limb
femoral artery supplying the lower limb
radial and ulnar arteries of the forearm
anterior and posterior tibial arteries of the leg
These arteries are particularly important for supplying skeletal muscles, bones, and joints of the limbs, where blood flow must be dynamically regulated during movement and physical activity.
Arterioles
Arterioles represent the smallest branches of the arterial system and function as the principal regulators of blood flow into capillary networks. Their walls contain only a few layers of smooth muscle cells, but these cells exert a powerful influence on vascular resistance.
By contracting or relaxing their smooth muscle layer, arterioles control the volume of blood entering capillary beds, thereby regulating tissue perfusion and systemic blood pressure. This mechanism is especially important in skeletal muscle, where arteriolar dilation significantly increases blood flow during physical activity to meet elevated metabolic demands.
Arterioles therefore play a central role in:
controlling peripheral vascular resistance
regulating systemic arterial pressure
adjusting local blood flow according to tissue metabolic activity
Capillaries
Capillaries are the smallest and most numerous vessels of the circulation, forming the microvascular interface between arterial inflow and venous return. Although not structurally part of the arterial tree, they receive blood from terminal arterioles and constitute the primary site of exchange between blood and tissues.
Structurally, capillaries consist of a single layer of endothelial cells with a basement membrane, optimized for minimal diffusion distance. This architecture enables efficient exchange of O₂, CO₂, nutrients, metabolites, hormones, and fluidvia diffusion, filtration, and transcytosis, governed by concentration gradients and Starling forces.
Within the musculoskeletal system, capillary networks perfuse skeletal muscle, bone, periosteum, tendons, ligaments, and fascia, supporting oxidative metabolism, tissue repair, and adaptation to mechanical load. In skeletal muscle, capillary density correlates with metabolic demand, increasing with endurance training to enhance oxygen delivery and mitochondrial function.
Capillaries are organized into capillary beds, where flow is dynamically regulated by precapillary sphincters and local metabolic control (e.g., hypoxia, ↑CO₂, ↓pH, adenosine). This ensures preferential perfusion of actively metabolizing tissues, particularly during exercise.
After exchange, blood is collected into venules,
initiating venous return to the heart
Description
Arterial anastomoses are direct vascular communications between two or more arteries supplying the same anatomical region. These connections form alternative pathways through which blood can reach tissues when the principal arterial route is narrowed, compressed, or obstructed. Within the musculoskeletal system, arterial anastomoses are particularly well developed around highly mobile synovial joints, where limb movement may transiently alter the patency of the main arterial supply.
Through these connections, collateral circulation may develop, allowing blood flow to be redirected through secondary vessels when the primary arterial pathway becomes compromised. In cases of gradual arterial occlusion, collateral vessels may enlarge and maintain adequate perfusion of distal tissues.
Important arterial anastomotic networks occur around the shoulder, elbow, hip, and knee joints, where multiple arterial branches interconnect to maintain continuous vascular supply during movement.
Scapular Anastomosis
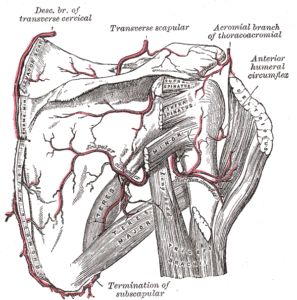
Scapular and Circumflex Arteries (Gray’s Anatomy Plate 521)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
The scapular anastomosis forms an important collateral pathway between branches of the subclavian artery and the axillary artery, ensuring blood supply to the upper limb if the proximal axillary artery becomes obstructed.
The principal arteries forming the scapular anastomotic network include:
Suprascapular artery – branch of the thyrocervical trunk from the subclavian artery
Dorsal scapular artery – usually a direct branch of the subclavian artery (sometimes arising from the transverse cervical artery)
Circumflex scapular artery – branch of the subscapular artery, which arises from the third part of the axillary artery
These vessels form a vascular network within the supraspinous and infraspinous fossae of the scapula, allowing blood from the subclavian circulation to reach the distal axillary artery.
Elbow Anastomosis
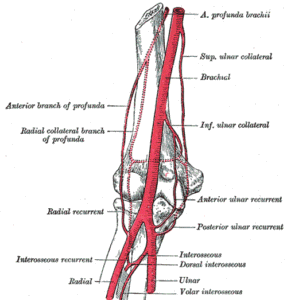
Arteries of the Arm (Gray’s Anatomy Plate 526)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
A rich arterial network surrounds the elbow joint, maintaining blood supply during flexion and extension when the main vessels may be partially compressed.
The elbow anastomosis is formed by descending collateral branches from the brachial artery and ascending recurrent branches from the radial and ulnar arteries.
Collateral arteries (descending)
Superior ulnar collateral artery – branch of the brachial artery
Inferior ulnar collateral artery – branch of the brachial artery
Radial collateral artery – branch of the profunda brachii artery
Recurrent arteries (ascending)
Radial recurrent artery – branch of the radial artery
Anterior ulnar recurrent artery – branch of the ulnar artery
Posterior ulnar recurrent artery – branch of the ulnar artery
Interosseous recurrent artery – branch of the posterior interosseous artery
These vessels form a periarticular network surrounding the humeroulnar and humeroradial joints.
Genicular Anastomosis
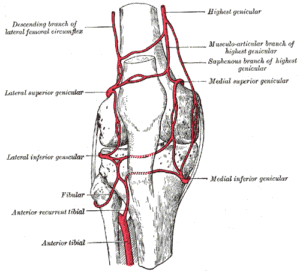
Genicular Anastomosis of the Knee (Gray’s Anatomy Plate 552)” – Henry Vandyke Carter, from Henry Gray’s Anatomy of the Human Body, Wikimedia Commons. Public Domain
The genicular anastomosis forms a dense vascular network around the knee joint, maintaining perfusion during joint flexion, extension, and weight-bearing.
The principal arteries forming the genicular network include branches of the popliteal artery, with additional contributions from the femoral and anterior tibial arteries.
Branches of the popliteal artery
Superior medial genicular artery
Superior lateral genicular artery
Inferior medial genicular artery
Inferior lateral genicular artery
Additional contributing arteries
Descending genicular artery – branch of the femoral artery
Descending branch of the lateral circumflex femoral artery
Anterior tibial recurrent artery – branch of the anterior tibial artery
These vessels form a vascular ring surrounding the capsule and ligaments of the knee joint.
Other Anastomosis
Trochanteric Anastomosis
The trochanteric anastomosis supplies the femoral head and neck and is particularly important for maintaining the vascular supply of the hip joint.
This arterial network is formed by:
Ascending branch of the medial circumflex femoral artery
Ascending branch of the lateral circumflex femoral artery
Superior gluteal artery
Inferior gluteal artery
These arteries form a vascular ring around the greater trochanter of the femur and contribute to the retinacular arteries supplying the femoral head.
Cruciate Anastomosis
The cruciate anastomosis lies posterior to the proximal femur and connects arteries of the internal iliac system with those of the femoral system.
The arteries involved include:
Medial circumflex femoral artery
Lateral circumflex femoral artery
Inferior gluteal artery
First perforating artery of the profunda femoris
This network provides collateral circulation between the internal iliac and femoral arterial systems.
Pulse Assessment
Arterial pulses represent the propagation of pressure waves through the arterial system and serve as a direct clinical indicator of downstream tissue perfusion. The presence, amplitude, and symmetry of pulses provide essential information about arterial patency, vascular integrity, and overall hemodynamic status.
Clinically, diminished or absent pulses suggest arterial obstruction or ischemia, while asymmetry indicates localized vascular compromise and bounding pulses reflect hyperdynamic circulation. As such, pulse assessment directly correlates with tissue viability, muscular performance, and the capacity for healing within the musculoskeletal system.
Anastomosis
Arterial anastomoses form interconnected vascular networks that provide alternative pathways for blood flow, ensuring continuity of perfusion when primary vessels are compressed or obstructed. This collateral circulation is particularly important in regions of high mobility, such as around joints, where vessels may be transiently occluded during movement.
Functionally, anastomoses maintain consistent blood supply under varying mechanical conditions and enable adaptive redistribution of flow. Clinically, they are critical in gradual arterial occlusion, where collateral compensation can preserve tissue viability; failure of these networks leads to ischemia, necrosis, and loss of function.
Functional Integration
Within the musculoskeletal system, arterial circulation is fundamental for sustaining mechanical performance and structural integrity. By delivering oxygen and metabolic substrates, it supports ATP production required for muscle contraction, facilitates tissue repair and remodeling, and contributes to joint function through synovial and subchondral perfusion. Furthermore, arterial supply enables adaptation to mechanical stress by supporting cellular turnover and structural reinforcement.
These processes collectively underpin endurance, load tolerance, and the capacity for functional recovery following stress or injury.
Clinical Integration
From an integrated clinical perspective, arterial function must be understood as a dynamic system combining real-time perfusion and collateral support. Pulses reflect the immediate adequacy of blood flow, while anastomotic networks provide a reserve mechanism that safeguards tissue perfusion under physiological and pathological conditions.
Movement capacity therefore depends on both sufficient arterial supply and continuity of flow. Impairment at either level compromises tissue survival, reduces mechanical efficiency, and limits recovery potential, emphasizing the central role of arterial circulation in musculoskeletal health and function.
Ischemia Tissue Viability
Disruption of arterial supply compromises continuous delivery of oxygen and metabolic substrates, leading to tissue ischemia and cellular dysfunction. Skeletal muscle and bone are highly metabolically active and therefore particularly vulnerable to reduced perfusion.
Prolonged ischemia results in ATP depletion, loss of ion homeostasis, and cellular necrosis, ultimately manifesting as functional impairment. Clinically, this underlies conditions such as arterial occlusion due to thrombosis, embolism, or atherosclerosis, where reduced blood flow leads to muscle weakness, pain, and potential tissue loss.
Vascular Injury
Trauma to arterial structures – whether from fractures, dislocations, or penetrating injuries—can directly compromise regional blood supply. Certain anatomical regions exhibit critical vascular dependence, where disruption of a single arterial source leads to severe consequences.
A key example is the femoral head, where interruption of its blood supply may result in avascular necrosis (AVN). This highlights the essential role of arterial integrity in maintaining bone viability and structural stability.
Compartment Syndrome
Compartment syndrome represents a pathophysiological state in which increased intracompartmental pressure exceeds capillary perfusion pressure, restricting arterial inflow and venous outflow. The resulting ischemia rapidly leads to muscle and nerve damage, making this a surgical emergency.
Without timely decompression, irreversible tissue necrosis and long-term functional loss occur, emphasizing the critical balance between vascular supply and mechanical constraints.
Surgical Rehabilitation
Preservation and restoration of arterial supply are central to clinical practice. In orthopedic and reconstructive surgery, adequate perfusion is essential for fracture healing, graft survival, and tissue regeneration. In sports medicine and rehabilitation, re-establishing vascular flow supports recovery, adaptation, and return to function. Consequently, detailed knowledge of arterial anatomy is fundamental for clinicians, as arterial integrity directly determines healing capacity, functional outcomes, and long-term musculoskeletal health.